

The UK-Public Health Rapid Support Team is a key international partner in infectious disease outbreak detection, prevention, preparedness and response; operational research; and capacity strengthening.
We are an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine, funded with UK aid by the UK Department of Health and Social Care.
About the team
The UK-Public Health Rapid Support Team is a key international partner in epidemic disease response. We partner with low- and-middle income countries to respond to infectious disease outbreaks before they develop into global health emergencies. We work closely with international organisations, partner country governments and non-governmental organisations to:
- Rapidly investigate and respond to disease outbreaks at their source in LMICs eligible for UK Official Development Assistance, with the aim of stopping a public health threat from becoming a broader health emergency.
- Conduct research to generate an evidence base for best practice in epidemic preparedness and response.
- Strengthen capacity for improved national response to disease outbreaks in LMICs
We are an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine, funded with UK aid by the UK Department of Health and Social Care.
Deployable team

The team responds to requests from national governments and multinational global health partners to deploy public health experts across multiple disciplines. The UK-PHRST is able to deploy rapidly and at short notice to support the prevention and control of infectious disease outbreaks, before they develop into global emergencies.
Support is provided in:
- Epidemiology
- Microbiology
- Infection Prevention & Control
- Risk Communication and Community Engagement
- Social science
- Mental Health and Psychosocial Support.
The team has deployed to outbreaks of multiple diseases including Ebola virus disease, COVID-19, Lassa fever, meningitis, cholera and plague
Deployment of the UK-PHRST is at the invitation of the host government or in response to requests made by the World Health Organization (WHO) or by the Global Outbreak Alert and Response Network (GOARN).
Reservist team
In addition to the core deployable team, the UK-PHRST has a group of public health reservists to ensure the UK is able to scale up its response to any disease outbreak or health emergency.
- Case study: UK-PHRST action against Lassa fever
Lassa virus causes a potentially fatal haemorrhagic fever syndrome that, in its most severe form, is similar to Ebola virus disease. The virus is carried by a rodent called the “multimammate rat”, which is found across West Africa, infecting humans exposed to infected rodent excreta, with occasional secondary transmission between humans, including to healthcare workers. There are estimated to be hundreds of thousands of infections and tens of thousands of deaths due to Lassa fever every year, with transmission usually peaking during the dry season.
Outbreak response: Putting out the fire
Lassa fever reached epidemic proportions in Nigeria during the dry seasons of 2018 and 2019, prompting the Nigerian Centres for Disease Control to request support from the UK-PHRST. The UK-PHRST quickly deployed personnel to provide epidemiologic, laboratory, and logistical support to Nigeria to help bring the outbreak under control.
Research: Identify the causes of the fire
The UK-PHRST is collaborating with investigators in Nigeria and Sierra Leone – two countries where Lassa fever is hyperendemic and often leads to epidemic spread – to fill key knowledge gaps regarding this dangerous disease. These include studies exploring the clinical evolution and pathogenesis of Lassa fever and looking at the pharmacokinetics of ribavirin, a drug used to treat the disease but whose efficacy and mechanism of action remains to be determined.
In the laboratory, the UK-PHRST is working on the development of a less invasive diagnostic antibody test that can be performed on saliva (as opposed to on blood), which will facilitate field studies on risk factors for transmission. The UK-PHRST is also engaged in social science research to better understand healthcare seeking behaviour for febrile illness in an effort to encourage early recognition and presentation of care for people with Lassa fever, potentially allowing rapid implementation of life-saving care.
Capacity building: Preventing future fires
With an eye to the long-term, the UK-PHRST is helping to development clinical research capacity at the Kenema Lassa Ward in Kenema, Sierra Leone, one of the major care centres for the disease in West Africa. This will facilitate the study of novel therapeutic agents and vaccines for Lassa Fever, with the hope of ultimately being able to prevent the disease. In addition to enhancing the physical infrastructure in Kenema, the UK-PHRST has sponsored the training of local physicians in the use of various techniques, such as echocardiography to assess cardiac function, to better understand the pathophysiology of Lassa fever, and thus provide better clinical care.
Background to the UK-PHRST

The Ebola crisis in West Africa in 2014/15 highlighted the need for the international community to develop a system to help countries respond to and control disease outbreaks that pose a threat to public health, before they develop into a global emergency.
The UK Public Health Rapid Support Team was developed as part of the UK contribution to global health security and to complement the World Health Organization’s work on the Global Health Emergency Workforce. The team is funded over five years by £20 million made available from the UK official development assistance budget. Former Public Health Minister Nicola Blackwood officially announced the launch of the team in November 2016.
The London School of Hygiene & Tropical Medicine was chosen to lead the UK-PHRST in partnership with Public Health England (now UK Health Security Agency).
LSHTM is one of the world’s leading public health universities. Its 3,500 staff and 4,700 students are working together to help create a more healthy, sustainable and equitable world for everyone. With main sites in London, The Gambia and Uganda, and an annual research income of £190 million, it is uniquely placed to make a tangible impact on people’s lives through highly-rated research, postgraduate education and global networks. LSHTM’s mission is to improve health and health equity in the UK and worldwide; working in partnership to achieve excellence in public and global health research, education and translation of knowledge into policy and practice.
Further information:
The UK-PHRST is an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine, funded with UK aid by the UK Department of Health and Social Care.

Ed Newman
UK-PHRST Director (UKHSA)
UK-PHRST Director (UKHSA)/Honorary Professor in the Practice of Global Outbreak Response, LSHTM

Shelley
Lees
Professor Anthropology of Public Health
UK-PHRST Deputy Director of Research (LSHTM)/Professor of Anthropology of Public Health, LSHTM

Thom Banks
UK-PHRST Programme Manager (LSHTM)

Babak Afrough
UK-PHRST Interim Programme Manager (UKHSA)
Cristina Leggio
Lead Microbiologist (UKHSA)
Anthony Twyman
IPC Team Lead (UKHSA)/Senior IPC Specialist (UKHSA)
Infection Prevention and Control Team Lead (UKHSA)/Senior Infection Prevention and Control Specialist (UKHSA)
Claire Bayntun
UK-PHRST Head of Capacity Strengthening (UKHSA)
UK-PHRST Head of Capacity Strengthening (UKHSA)/Honorary Clinical Consultant, Global Leadership Programmes, LSHTM
Victor Del Rio Vilas
Epidemiology Co-lead (UKHSA)
UK-PHRST Epidemiology Co-lead (UKHSA)/Senior Epidemiologist (UKHSA)
UK-PHRST Epidemiology Co-lead (LSHTM)

Farhana
Haque
Assistant Professor
UK-PHRST Implementation Science lead (LSHTM)/Assistant Professor, LSHTM
James
Hargreaves
Professor in Epidemiology and Evaluation
Professor of Epidemiology and Evaluation (LSHTM)

Nadine
Beckmann
Associate Professor in Social Science
UK-PHRST Social Science Lead (LSHTM)/Associate Professor in Social Science (LSHTM)
Shelley
Lees
Professor Anthropology of Public Health
Professor of Anthropology of Public Health, LSHTM

Professor Julian Eaton
UK-PHRST Mental Health and Psychosocial Team lead/ Professor of Global Mental Health, LSTM
UK-PHRST Mental Health and Psychosocial Team lead/ Professor of Global Mental Health, LSTM
Ed Newman
UK-PHRST Director (UKHSA)
UK-PHRST Director (UKHSA)/Honorary Professor in the Practice of Global Outbreak Response, LSHTM
Richard Amlôt
Scientific Programme Leader, Behavioural Science (UKHSA)
Miles Carroll
University of Oxford
Jake Dunning
Senior Clinical Research Fellow in Emerging and High Consequence Infectious Diseases (University of Oxford)
Martin Hibberd
Professor of Emerging Infectious Disease (LSHTM)

Adam
Kucharski
Professor of Infectious Disease Epidemiology
Shelley
Lees
Professor Anthropology of Public Health
TSC Chair
Mohammed Abdulaziz
Head of Disease Control and Prevention (Africa CDC)
Nigel Field
Director of the Centre of Molecular Epidemiology and Translational Research at the Institute for Global Health (UCL)
Thom Banks
UK-PHRST Programme Manager (LSHTM)
E. Wangeci Kagucia
Research Fellow, KEMRI Wellcome Trust
William Nicholas
UK-PHRST Project Manager (LSHTM)
Stella Atim
Senior Veterinary Officer, Animal Disease Diagnostics and Epidemiology, Ministry of Agriculture Uganda
Jonas Brant
Professor of Public Health, University of Brasilia
Cristina Leggio
Lead Microbiologist (UKHSA)
Adeyinka Adedeji
Veterinarian at National Veterinary Institute, Vom, Nigeria

The UK Public Health Rapid Support Team (UK-PHRST) receives requests for deployment through WHO-GOARN, direct requests from the government of the state affected by the epidemic, or through the UK Emergency Medical Team and DFID.
The first deployment of the UK-PHRST took place in April-May 2017, when two epidemiologists and one clinical researcher deployed through GOARN to the Somali Regional State of Ethiopia to support an escalating outbreak of acute watery diarrhoea.
This was followed in May-June 2017 by a deployment through GOARN to Nigeria when a team of two epidemiologists and one laboratory microbiologist assisted in the response to an outbreak of cerebral meningitis.
The UK-PHRST’s first bilateral deployment was to Sierra Leone (August-September 2017) when two epidemiologists, two microbiologists, one logistician, two Field Epidemiology Training Programme (FETP) fellows and the UK-PHRST Director were deployed. In this instance they assisted in the establishment of water-borne disease surveillance and assessment of diagnostic capacity at Connaught Hospital in Freetown in the wake of heavy rains, flooding and landslides in and around the capital.
In October – November 2017, two epidemiologists and one clinician were deployed to Madagascar though GOARN to support the response to an outbreak of pneumonic plague affecting primarily two large urban centres.
This was followed by a deployment to Bangladesh (December - January 2017/18) when a team consisting of an epidemiologist, a FETP fellow and an Infection Prevention Control (IPC) specialist worked alongside the UK Emergency Medical Team and DFID in support of the international response to the outbreak of diphtheria in the displaced Rohingya population in refugee camps in Cox’s Bazar.
The second bilateral deployment came in February-March 2018 in Nigeria, when an epidemiologist, FETP fellow, case management specialist and a logistician supported the government in controlling a large outbreak of Lassa fever through field-level interventions, logistics, capital-level data analysis and intervention strategy. This fostered a good partnership between UK-PHRST and Nigeria Centre of Disease Control (NCDC). In February-March 2019, UK-PHRST were invited to support the control of the a Lassa fever outbreak in Nigeria once more.
During February – March 2018, two epidemiologists and one infection prevention and control specialist were deployed to Bangladesh once again to support the WHO response to surveillance and monitoring of infectious disease outbreaks in the Rohingya refugee camps in Cox’s Bazar. In July 2018 an IPC specialist was redeployed to Cox’s Bazar.
In May-June 2018 during the Ebola outbreak in DRC, UK-PHRST deployed two epidemiologists and a data scientist to support with strengthening the alert system, including case investigation, protocol development, epidemiological analysis and data management.
The UK-PHRST is still actively engaged in the ongoing Ebola outbreak in DRC and has been instrumental in providing senior epidemiological support and in setting up the analytical cell, which is fully operational at the strategic coordination level (currently in Goma).
In 2019, deployments of UK-PHRST epidemiologists, data scientists and IPC specialist in response to the Ebola outbreak in DRC, have been continuous through GOARN.
At the end of March 2020, UK-PHRST in-person deployments to Africa CDC (Ethiopia), WHO Western Pacific Regional Office (the Philippines) and WHO Nepal to support the response to the emerging COVID-19 outbreak were cut short. This was due to the abrupt cessation of flights and rapid closure of borders globally. Despite the rapid change in location, the teams quickly adapted to remote working, continuing the support they had initiated with colleagues overseas.
This coordinated package of remote support has continued alongside in-person deployments when possible, subsequently benefiting from the team’s ability to draw on additional expertise from the pool of reservists and extended team when required.
Summary of Key COVID-19 Response Activities
Africa CDC
Initially an epidemiologist, infection prevention and control (IPC) specialist, social scientist and microbiologist were engaged directly at the Africa Centres for Disease Control and Prevention (Africa CDC) headquarters in Ethiopia. Since their return to the UK, a comprehensive programme of remote support has continued. Key areas include:
- Epidemiology
- Infection prevention and control
- Laboratory
- Social science
Bangladesh
We continue to build on previous UK-PHRST deployments as well as remote support to WHO’s Sub Office in Cox’s Bazar, with support from Field Epidemiology Training Programme (FETP) Fellows and UK-PHRST reservists. Key areas include:
- Epidemiology and data science
- Infection prevention and control
- Laboratory
- Research - Read about the COVID-19 seroprevalence study
Read more: UK Public Health Rapid Support Team COVID-19 Response – Bangladesh
WHO African Regional Office
One UK-PHRST field epidemiologist and two data scientists assisted WHO AFRO with analysis and interpretation of data gathered from across member states. The team supported WHO AFRO remotely and provided brief reports on the data that different countries had provided.
WHO Country Office (WCO) Tajikistan
In June, the UK-PHRST deployed one microbiologist and one epidemiologist on an assessment mission to determine the appropriateness, feasibility and likely impact of deployment of a Rapid Response Mobile Laboratory (RRML) to support the COVID-19 response. This was in response to a request for support through the Global Outbreak Alert and Response Network for the Tajikistan Ministry of Health and Social Protection in response to increasing case numbers of COVID-19.
The Gambia
Following a joint rapid assessment on COVID-19 response with colleagues from Africa CDC, UK-PHRST deployed a team of four to support the scaling up of testing and contact tracing services and the improvement of data systems. This was a bilateral deployment in collaboration with the Ministry of Health with support from two epidemiology specialists and two laboratory experts, all of whom have now returned to the UK and will continue to engage remotely.
Read more: COVID-19 Surveillance in The Gambia
Strengthening public mental health in Africa in response to COVID-19
Globally, mental health faces unprecedented challenges due to COVID-19. Bereavement, isolation, loss of income and fear are triggering mental health conditions or exacerbating existing ones. National leaders face significant challenges in protecting and scaling up mental health support as part of the COVID-19 response. A recent WHO global survey indicated that 37% countries reported that COVID-19 mental health response plans were only partially funded and a further 37% reported having no funds at all.
The UK-PHRST “Strengthening public mental health in Africa in response to COVID-19” project, due for completion in March 2021, aims to better understand enablers and barriers to integrating mental health and psychosocial support (MHPSS).
Read more: UK-PHRST Strengthening public mental health in Africa in response to COVID-19

The UK-Public Health Rapid Support Team has co-created a global multi-disciplinary research programme to support and improve the effectiveness of infectious disease outbreak response in Official Development Assistance (ODA) eligible countries.
Our research priorities are co-identified with partners in ODA eligible countries and the research aims to provide evidence for improving practice across the following five themes:
- Preparedness and prevention
- Detection
- Response
- Impact and evaluation
- Operational research
We work across research disciplines covering epidemiology, microbiology, clinical and veterinary sciences, infection prevention and control, social sciences, mental health, implementation science, modelling and One Health.
We aim to improve the impact of our research through effective community engagement and the formation of South-South and cross-border collaborations. We also provide expertise, training and technology transfer to strengthen research capacity in partner countries.
Our research projects
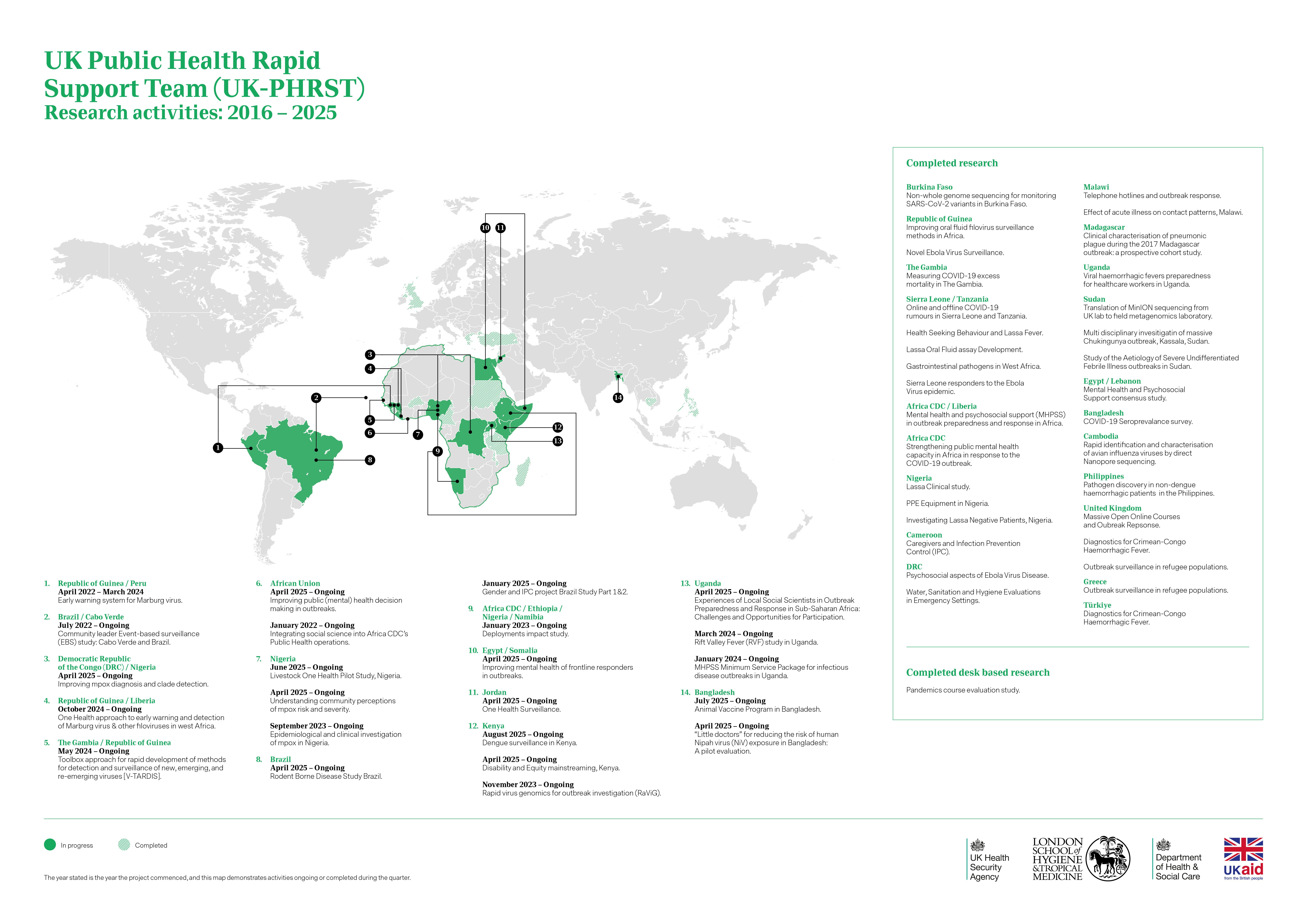
Since 2016, UK-PHRST has delivered 52 research projects, spanning 20 low- and middle-income countries. See below for more information on our active research projects in collaboration with our partners.
Active research projects
- Outbreak preparedness and prevention
Outbreak preparedness and prevention focuses on developing strategies, tools, and systems to anticipate, prevent, and effectively respond to infectious disease outbreaks to minimise their impact on public health.
Rapid Virus genomics for outbreak investigation (RaViG) - proof of principle in coastal Kenya

The project assesses whether deploying portable whole genome sequencing (WGS) in real-time during outbreaks is feasible, and if this provides added value to conventional outbreak response approaches.
This research is particularly important for the coastal Kenya region which has experienced recurrent outbreaks of viral diseases including dengue, measles, norovirus, influenza, and COVID-19 in recent years. However, implementation of real-time portable sequencing during outbreaks would require substantial investment to sustain capacity, maintain trained staff and replenish key resources. Therefore, it is important to generate evidence on the added value, costs and feasibility of using real-time sequencing during outbreak response, and whether it improves our understanding of how outbreaks begin and spread in these communities.
Researchers are comparing the feasibility and sustainability of using in-field rapid genomic sequencing compared to conventional surveillance in low resource settings. Ultimately, this will allow them to potentially use the findings to influence policy or outbreak control measures. The study team are also working with the Kenyan Ministry of Health, Africa Centres for Disease Control (CDC), and the Regional World Health Organization office to develop tools and resources to guide appropriate application of portable WGS.
Read more about this project on our UK-PHRST Global Health Network site.
Epidemiological and clinical investigation of mpox in Nigeria: A multi-disciplinary research project to inform case management and outbreak prevention and control
Researchers from the Nigeria Centre for Disease Control (NCDC) and UK-PHRST have teamed up with Nigerian and UK partners to increase understanding of how mpox spreads and affects communities in Nigeria. The UK-PHRST is collaborating with Nigerian partners in the co-ordination and implementation of the study in two states in Nigeria, as well as lab capacity strengthening and data analysis.
The project will help address the current significant gaps in clinical and epidemiological knowledge of the virus in Nigeria. Its findings have the potential to not only strengthen detection, prevention, response, and control in Nigeria, but also inform practice in other countries across the world where mpox is endemic.
Read more about this project on our UK-PHRST Global Health Network site.
Integrating Social Science into Africa CDC’s Public Health Operations

Following interest expressed by Africa CDC in increasing the use and integration of social science across its operations and staff skillset, this project aims to explore and understand the status of social science at Africa CDC and to identify key operational steps to integrate social science into its current and future public health preparedness and response activities. The project also seeks to understand the barriers and opportunities to integrating social science and to identify strategic areas to increase its use within Africa CDC. To achieve this, the researchers have temporarily integrated themselves into Africa CDC’s daily operations, discussions with key staff members to build a picture of the organisation’s culture and approach to social sciences.
The project’s findings will help create a roadmap for social science integration for Africa CDC’s immediate use.
Understanding the public health threat of rodent-borne viruses in Brazil's Atlantic Forest

Researchers from Fiocruz in Rio de Janeiro and UK-PHRST are studying rodent-borne viruses in Brazil's Atlantic Forest, where urban expansion is bringing people into closer contact with wildlife. The study focuses on Rio Claro municipality, where rodents known to carry arenaviruses and hantaviruses are present. The team will trap rodents, sequence their viruses, and test blood samples from local patients with unexplained fevers to assess the scale of human exposure. They will also engage local communities and healthcare workers to build awareness and practical guidance. The project will deliver new diagnostic tools and surveillance methods that can be shared with Brazilian health authorities and international networks in the event of a future outbreak.
Read more about this project on our UK-PHRST Global Health Network site
- Outbreak detection
Outbreak detection focuses on developing and refining methods and technologies to quickly identify the emergence and spread of infectious diseases to enable timely and effective public health interventions.
Toolbox approach for rapid development of methods for detection and surveillance of new, emerging, and re-emerging viruses [V-TARDIS]
![Toolbox approach for rapid development of methods for detection and surveillance of new, emerging, and re-emerging viruses [V-TARDIS], Discipline: Microbiology, Lead Academics: Dr David J Allen, Dr Abdul Sesay, Dr Joseph Akoi BORE , Cristina Leggio, Sonal Shah, Countries: UK, Guinea, The Gambia, Collaborators: Centre de Recherche et d'Analyse Médicale (CRAM), Guinea, Dates: May 2024 – Ongoing](/sites/default/files/V%20Tardis%20info%20card.png)
This project aims to tackle a key disease outbreak response problem: the need for diagnostics and surveillance infrastructure in low resources countries.
Using both a review of the latest literature and open dialogue with partners, the project will provide a current view of challenges, resources, and gaps in preparedness faced by low resource countries.
The project is working to develop a ‘toolbox’ for a specific virus by creating a suite of readily available and reliable diagnostic tools for countries that would benefit from them most.
This ‘toolbox’ approach could be generalised to support low-resource countries and settings to rapidly identify methods for detection and surveillance of other new, emerging, and re-emerging viruses– improving their outbreak detection and surveillance abilities.
Read more about this project on our UK-PHRST Global Health Network site.
Effectiveness of early warning systems involving local community leaders for early detection of health-related events indicative of outbreaks: A pilot in Cabo Verde and Brazil
The Guardians of Health Event based surveillance Community Leaders project, based in Brazil and The Republic of Cabo Verde, aims to develop a new early warning system for health-related events involving the active contributions of community leaders.
The study is investigating whether a community-led event-based surveillance (EBS) system is feasible and more effective at detecting outbreaks of infectious disease than conventional systems without direct community participation. It also aims to understand how sustainable this approach could be, and whether the involvement of community leaders in the design of the data reporting system from the beginning can help enhance local health surveillance in the longer-term.
Once concluded, the EBS trialled as part of the study will be evaluated with community leaders and local surveillance and public health teams to understand its impact on public health action in the communities. The team will produce recommendations for suggested changes to the EBS and how the system could be used in the long-term in Brazil and Cabo Verde, and potentially replicated in other low-and-middle income countries.
Read more about this project on our UK-PHRST Global Health Network site.
- Outbreak response
Outbreak response focuses on creating and optimising strategies, resources, and actions to effectively contain, mitigate, and manage infectious disease outbreaks once they have been detected.
A participatory study to identify gaps and solutions to zoonotic disease detection and reporting: A case study of Rift Valley Fever in Kalunga District, Uganda
This project is working to understand the gaps in outbreak detection and surveillance that lead to viruses spreading from animals to humans.
Rift Valley Fever (RVF) is a virus that poses a continuous threat to both animals and humans. This study is using RVF in Uganda as a real-world example where recurrent outbreaks occur to study how livestock keepers recognise sick animals, and how they are reported and treated by veterinary specialists. By doing this, the team hope to better understand how diseases that have the ability to spread from animals to humans can be better prevented and detected. The findings of this study aim to create actionable recommendations for policy makers and the development of programs to tackle animal-borne diseases.
Read more about this project on our UK-PHRST Global Health Network site.
Implementing the MHPSS Minimum Service Package for infectious disease outbreaks in Uganda - an evaluation study
Mental Health and Psychosocial Support (MHPSS) is a vital but often neglected, part of outbreak response measures and research. This project is looking to develop and evaluate a suite of tailored MHPSS interventions supporting outbreak preparedness and response in Uganda using the existing the Minimum Service Package (MSP) toolkit for MHPSS.
The project aims to identify and implement a package of MHPSS interventions for infectious disease outbreaks and test out if this is a feasible and acceptable approach in Uganda. If successful, the project aims to integrate MHPSS within outbreak planning and response at the national level and have a real-life positive impact on the mental health those affected by disease outbreaks.
Read more about this project on our UK-PHRST Global Health Network site.
- Impact and evaluation
Impact and evaluation involves assessing the effectiveness, outcomes, and broader implications of public health interventions and policies to inform future strategies and improve health systems overall.
Impact of international public health deployments on national outbreak preparedness and response in ODA-eligible countries
This project aims to evaluate international deployments to Overseas Development Assistant (ODA)-eligible countries to understand their impact on outbreak preparedness and response in the receiving country. It is exploring what, if any, difference is made and how this is achieved. It is also examining whether the impact of an ‘external’ expert on a country’s outbreak response is sustainable beyond the conclusion of the deployment.
To understand this, the team conducted a literature review followed by face-to-face interviews, an online survey, in-country case studies and online interviews with key national stakeholders in ODA-eligible countries to understand their perspectives on deployments and whether they are beneficial or a hinderance to their country’s overall national outbreak response capabilities.
The evaluation aims to provide evidence for learning opportunities for both ODA-eligible countries and external international deployment teams to inform ways of responding, as well as improve the impact and sustainability of future deployments.
Read more about this project on our UK-PHRST Global Health Network site.
Disability mainstreaming in the Kenyan public health system: Addressing equity during outbreak response
This co-led study is working with people with disabilities to improve the reach and reduce the harm of outbreak response measures in Kenya. Although the Kenyan government has laws and plans to support healthcare access and provision for people with disabilities, our Kenyan research partners find that these measures are often not implemented during acute disease outbreaks – leaving people with disabilities at increased risk during health emergencies.
To gather insights, the research team will conduct interviews and focus groups with people with disabilities, caregivers, responders, and policymakers. Alongside this, they will undertake a scoping review of global literature on the group’s experiences during disease outbreaks and review existing data and documents on past outbreak responses.
Ultimately, the researchers hope that by pinpointing the needs of people with disabilities during disease outbreak and identifying gaps in Kenya’s current health emergency response system, they will develop a plan for improving the reach and reducing the unintended harm of outbreak response measures for people with disabilities across Kenya.
Read more about this project on our UK-PHRST Global Health Network site.
- Operational research
This research theme is for projects that address questions that have arisen through deployments and/or urgent partner requests, the UK-PHRST is open to receiving applications for these types of research projects as and when they arise.

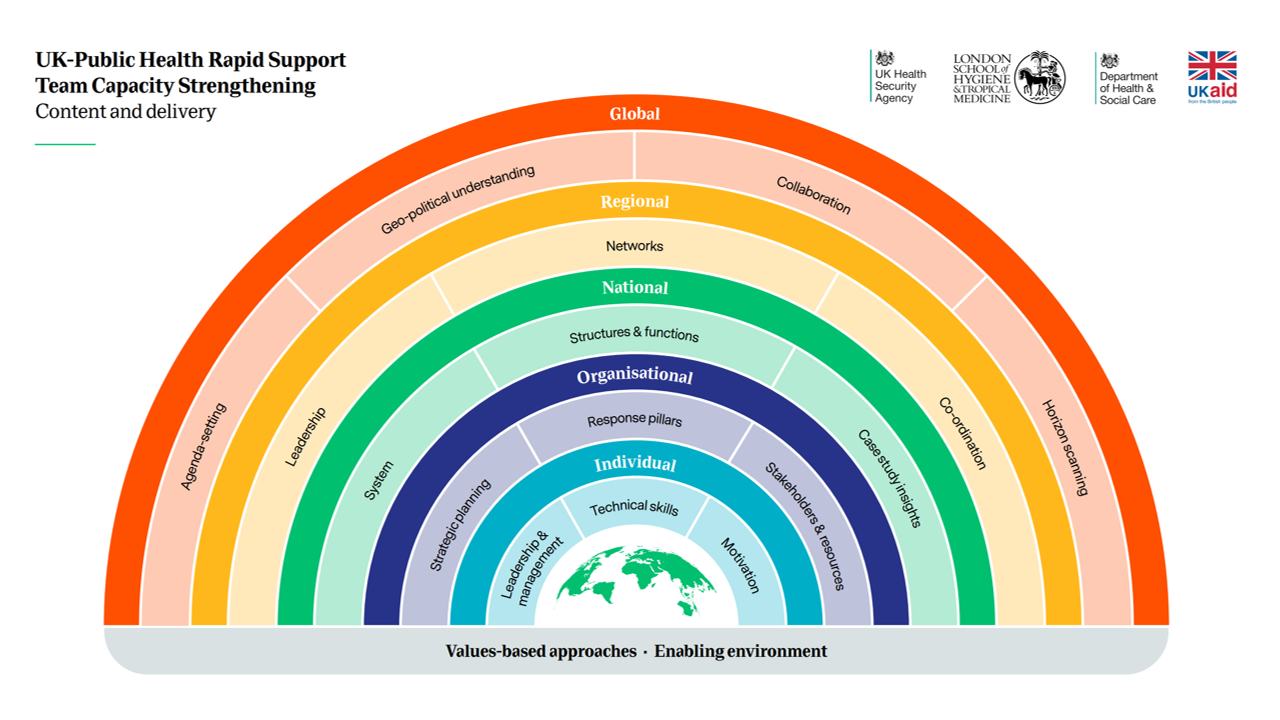
The UK Public Health Rapid Support Team (UK-PHRST) works alongside partners in low-resource countries to strengthen capacity for improved and rapid response to disease outbreaks. We work with global, regional, and national partners, focusing on technical collaboration, emergency coordination and systems for outbreak preparedness and response.
Our approach
We recognise that capacity strengthening is not one-size-fits-all: It must be tailored, contextualised and locally owned.
We co-design, co-develop and co-deliver initiatives with our partners, supporting implementation across all levels of the health system — from individuals and organisations to national structures and regional networks.
Our approach is guided by values-based principles and an enabling environment, and includes:
- Applied Learning – Practical, context-specific learning that is directly transferable to outbreak settings
- Equity and Inclusion – Embedding principles of social equity, diversity, and human rights in all activities
- Global Engagement – Serving as a credible and trusted voice in global capacity strengthening discussions
- Impact – Prioritising measurable outcomes that strengthen outbreak preparedness and response
- Partnerships – Collaborating through mutual trust, respect, and accountability to ensure inclusive, effective capacity strengthening
Sustainability – Supporting long-term system resilience by building on local capabilities and fostering knowledge exchange
Our projects
Our work is guided by six strategic themes:
- Community Protection
- Emergency Coordination Leadership
- One Health
- Planetary and Climate Health
- Research Capacity Strengthening
Technical Assistance
See below for a map showcasing all of our capacity strengthening projects since April 2025.
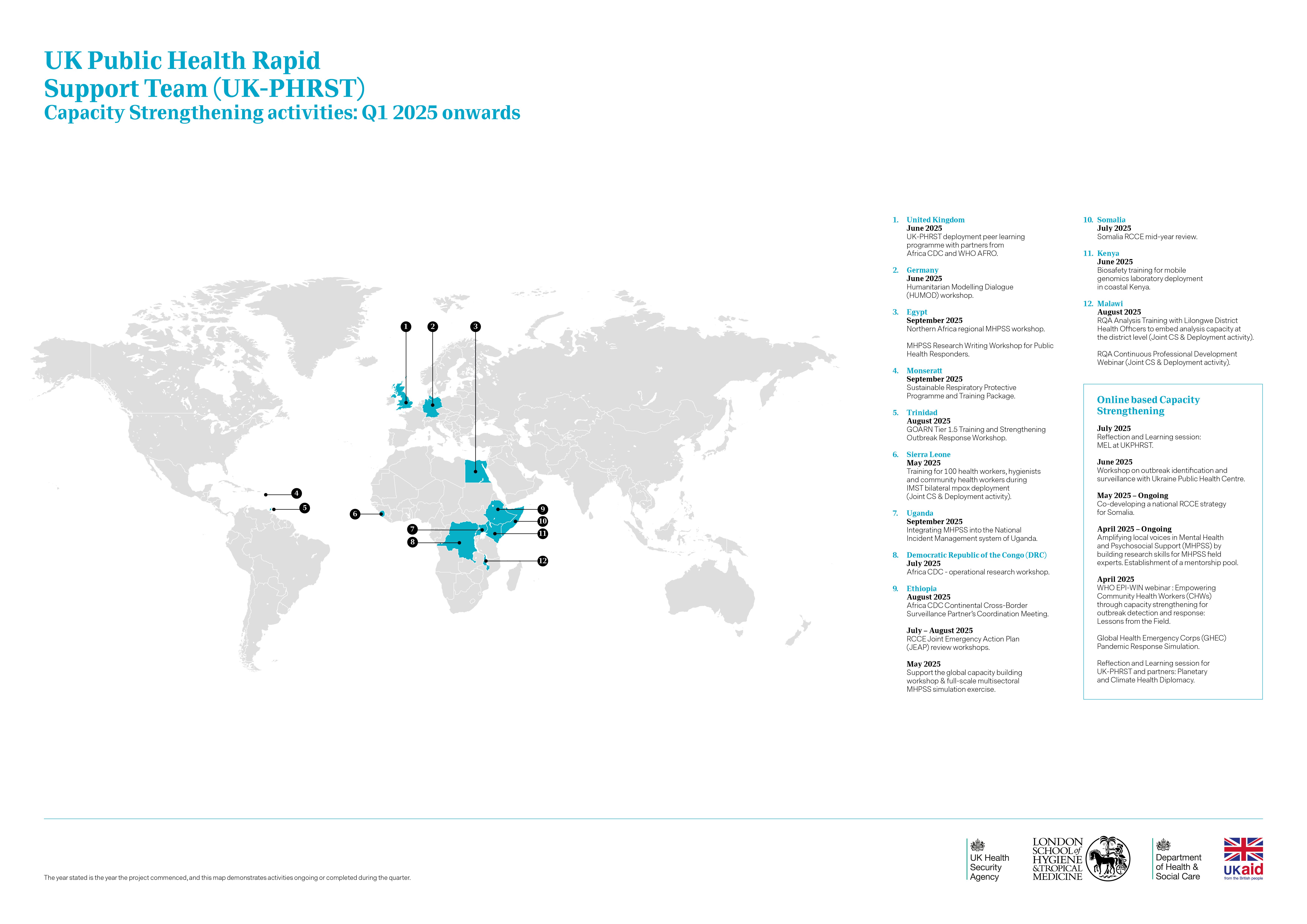
See our map showcasing all of our capacity strengthening projects between 2016 - 2025
Our work in action: Community readiness tabletop exercise, Ghana
In Feburary 2024, a three-day community readiness simulation exercise was co-organised by the Ministry of Health, Ghana, the World Health Organization and the UK-PHRST.
The exercise, the first to be conducted in Ghana, brought together 65 participants from three communities across two districts in the Eastern Region alongside stakeholders from health, local government, disaster management, animal and environment sectors.
It was aimed at enabling stakeholders to identify strengths, gaps and reflect on priorities that will help strengthen communities’ readiness, working with the health workforce to detect, notify and respond to public health threats before they escalate.
The exercise in Ghana provided valuable information to inform the WHO Community Readiness Checklist, including transferable lessons for other communities and countries.
As a result of the Ghana exercise:
- UK-PHRST/WHO developed a training package for community health workers/volunteers addressing specific disease outbreak characteristics, at-risk populations, community-based surveillance, home care, risk communication and community engagement, MHPSS and community care coordination. The training can be tailored to specific outbreaks.
- UK-PHRST/WHO developed a Train the Trainer package to support countries experiencing disease outbreaks, which was used during the mpox outbreak in the Democratic Republic of the Congo in January 2025, and the Ebola virus outbreak in Uganda in February 2025, delivered for both countries.
Our resources
We offer free, open-access resources to support deployment, capacity strengthening and applied research in:
- Emergency Outbreak Co-ordination
- Epidemiology
- Infection Prevention & Control
- Mental Health & Psychosocial Support
- Microbiology
- Planetary and Climate Health
- Research Capacity Strengthening
- Social Equity and Human Rights
- Social Sciences and Risk Communications and Community Engagement (RCCE)
View our resources on The Global Health Network Platform
Collaboration and technical support
We also welcome opportunities to collaborate on initiatives that support global health security through sustainable capacity strengthening.
At the request of partners, our team can provide sustainable capacity strengthening support in different expertise areas; epidemiology; microbiology; infection prevention and control; risk communication and community engagement; social science; and mental health and psychosocial support.
Email [email protected] to enquire about the UK-PHRST
UK-PHRST supports formation of Rwanda RCCE surge team for outbreak response
In February UK-PHRST supported a five-day training to set up a national Risk Communication and Community Engagement Surge Team in Rwanda who can be deployed during outbreaks.
This initiative, in collaboration with UNICEF and Rwanda Biomedical Centre, will ensure the country can respond quickly outbreaks in real time, ensuring communities are informed, engaged and at the centre of response efforts.
The workshop was a result of several successful UK-PHRST social science deployments to Rwanda during recent Marburg and mpox outbreaks and demonstrates that through good capacity strengthening work, the global health community can stop outbreaks spreading beyond borders while safeguarding local communities at the same time.
Integrating local social scientist perspectives into outbreak response

Over 50 experts from across LSHTM and social scientists from Uganda, Zambia and Ethiopia, Sierra Leone and Senegal gathered for a roundtable discussion to identify barriers that currently prevent social scientists being actively and meaningfully involved outbreak preparedness and response and to develop opportunities to solve this issue.
The roundtable is part of an ongoing UK-PHRST research project that has included a mapping exercise and in-depth interviews with local social scientists from across sub-Saharan African countries including Uganda, Zambia and Sierra Leone. During the event, the researchers shared their initial findings and, following discussions, worked to co-produce a strategic roadmap and country specific outreach plans to ensure the findings reach relevant audiences in country.
Implementing the road map will help amplify the voices of social scientists and take concrete steps towards integrating their expertise into outbreak response systems across sub-Saharan Africa.
Predicting the impact of outbreaks and public health measures on mental health

Academics from across LSHTM and research partners held a workshop in London to advance their work to develop a mathematical model to predict the impact of infectious disease outbreaks and resulting public health interventions on mental health.
The workshop is part of the ongoing UK-PHRST research project which aims to provide a framework for decision makers like Ministries of Health to better understand the potential impacts on mental health of disease outbreak control measures like social distancing and self-isolation. The researchers hope that this model will help shift practice and policy, to ensure outbreak response measures not only consider the physical health needs but also the psychological wellbeing of affected communities.
UK-PHRST and KEMRI Wellcome Trust Research Programme study demonstrates that portable whole genome sequencing is feasible during outbreak response

Researchers shared the findings of the joint research project Rapid virus genomics for outbreak investigation (RaViG) - proof of principle in Coastal Kenya at a dissemination event in Mombasa Kenya on 25 March 2026. The study found that portable genome sequencing is a feasible approach to curbing outbreaks in real-time as it accelerates source tracing and effectively strengthens county rapid response capacity.
The findings were shared with partners including the Kenya Ministry of Health, six coastal Kenyan counties and other study stakeholders. Workshop participants also discussed how to make the approach sustainable, ensure policy uptake and how to integrate in-field sequencing into routine public health surveillance.
Find out more about the project
Study to enhance Dengue fever surveillance kicks off in Mombasa and Machakos
Alongside the Kenya National Public Health Institute (NPHI), UK-PHRST held a training workshop for local research assistants in Mombasa and Machakos as part of the research study; An assessment to improve understanding of dengue surveillance capabilities in Kenya.
The workshop equipped researchers with the skills to undertake stakeholder interviews and design a survey exploring dengue fever related health-seeking behaviour, challenges facing the national health service, and national disease surveillance capacity.
The study aims to address a critical gap in dengue surveillance identified by Kenya NPHI, to enhance surveillance mechanisms and community engagement and improve outbreak detection, accelerate response and reduce lives lost.
UK-PHRST supports training for healthcare workers to look after their mental health during public health emergencies
In February 2026, the Somalian Ministry of Health, with support from UK-PHRST, held a mental health and psychosocial support (MHPSS) workshop for the country’s healthcare workers.
The workshop focused on how healthcare workers understand their own mental health needs, how to recognise stress and burnout, and self-care practices and mental health first aid principles.
The co-led research project Improving the mental health and wellbeing of Health workers in the context of infectious disease outbreaks and other health emergencies in the Eastern Mediterranean Region plays an important role in shining a light on the mental health challenges faced by healthcare workers in outbreaks. They are more likely than the general population to develop depression, anxiety, insomnia and trauma-related symptoms. Their needs are often sidelined due to workload demands, limited resources and a lack of coordination.
The research hopes to help national Ministries of Health in the region consider health workers' wellbeing in their outbreak preparedness and response plans, safeguarding the wellbeing of key professionals.
Metagenomics training to help Brazil better understand the threat from rodent-borne viruses

UK-PHRST microbiologists provided training to researchers at the Oswaldo Cruz Institute (Fiocruz) in Rio de Janeiro on genetic sequencing methodologies to expand the potential for detecting pathogens in rodent samples.
The co-led research project aims to create new diagnostic tests capable of detecting rodent-borne viruses circulating in Brazil which be available to Brazilian health authorities, WHO Collaborating Centres and international laboratory networks should an outbreak occur in the future. The team will also establish methods for ongoing surveillance that can be maintained after the project ends.
The UK Health Security Agency (UKHSA) is deploying public health specialists from the UK Public Health Rapid Support Team (UK-PHRST) to the Ebola outbreak in the Democratic Republic of Congo (DRC) and across the region.
Developed following the 2014 to 2015 West Africa Ebola outbreak and funded by the Department of Health and Social Care’s Official Development Assistance (ODA) budget, UK-PHRST works with low- and middle-income countries to respond and prepare for infectious disease outbreaks and public health emergencies. UK-PHRST brings extensive experience to the current response, including 10 deployments to Eastern DRC during the 2018 to 2019 North Kivu Ebola outbreak – part of more than 50 deployments involving over 100 people in the last 9 years.
As a key international partner in epidemic disease response, the team is now deploying 7 specialists from the UK Health Security Agency (UKHSA) and the London School of Hygiene and Tropical Medicine (LSHTM) to support the international response to the outbreak:
- 4 will be based in Eastern DRC, supporting World Health Organization (WHO) field operations across infection prevention and control, epidemiology, and risk communication and community engagement (RCCE)
- a further RCCE specialist is being deployed to the WHO country office in Kinshasa
- an epidemiologist is being deployed to the Republic of Congo to support the wider regional response
- additional support is being provided remotely by a data modelling expert
UK-PHRST has worked closely with WHO and UNICEF, offering support in response to the formal requests for assistance through the Global Outbreak Alert and Response Network (GOARN).
Today, UKHSA together with continued funding from the Department of Health and Social Care (DHSC) and in partnership with the National Institute for Health and Care Research (NIHR) also announced the renewal and expansion of the academic partnership underpinning the UK-PHRST more broadly.
The London School of Hygiene and Tropical Medicine will lead a new multi-institutional academic consortium, building on nearly a decade of collaborative research between UKHSA and LSHTM since the UK-PHRST was established in 2016. The expanded partnership brings together world-leading expertise in epidemic preparedness and response, with a central commitment to shared leadership between UK and low- and middle-income country (LMIC) institutions.
The £18million 5-year programme will conduct applied research across Africa and Southeast Asia, spanning the readiness, detection and response phases of epidemic outbreaks. Research priorities include equity and gender in outbreak response, mental health and psychosocial support, diagnostics, AI-assisted decision-making, and community engagement. Amid an increasing risk of epidemic threats, this renewal highlights the UK government’s commitment to global health security.
Dr Edmund Newman, Director of the UK Public Health Rapid Support Team at UKHSA, said:
This deployment will help strengthen the existing response to the Ebola outbreak in the DRC and across the region, with experts in epidemiology, risk communications and community engagement, infection prevention and control and data modelling now on the ground to support.
We know infectious diseases are not restricted by borders, which is why it’s vital we continue to work collaboratively with the World Health Organization and other international partners, as well as national and local response organisations, to protect global health security.
Amid uncertainty in the global landscape, we’re really pleased to announce the renewal and expansion of the UK-PHRST partnership with the London School of Hygiene & Tropical Medicine, which allows us to continue sustainably sharing knowledge and support internationally, delivering cutting edge research and evidence to help prevent outbreaks from becoming global health emergencies.
Jenny Chapman, Minister for Africa and International Development, said:
Ebola is a devastating disease, and this latest outbreak is deeply concerning. The UK is acting fast, working with regional partners to save lives and stop the spread.
The UK Public Health Rapid Support Team brings world-class expertise, from infection control to community engagement and modelling the data. It demonstrates our commitment to global health security, and supporting the African-led response to this crisis.
We are investing in the research, evidence and local leadership needed to respond faster and more effectively to this deadly disease.
The UK has committed up to £21 million to support the government-led Ebola response in DRC to support a locally led response, helping to protect frontline workers and vulnerable communities.
Today (16 June) the Minister for Africa and International Development will join African leaders, the WHO Director-General, the Africa Centres for Disease Prevention Director-General and others at their high level meeting to discuss regional preparedness and response.
UKHSA continues to monitor the Ebola outbreak closely. The risk to the public in the UK remains very low.

As part of the wider UK Government response to the hantavirus outbreak, the UK Public Health Rapid Support Team (a partnership between LSHTM and the UK Health Security Agency), has deployed a rapid response mobile laboratory (RRML) and three UKHSA staff members to the British Overseas Territory of St Helena.
The team includes two microbiologists who will provide PCR testing for hantavirus on the island, as well as supporting local testing to exclude other conditions. An infection prevention and control (IPC) expert will also support Jamestown General Hospital to prepare and respond to any potential cases, providing IPC assessments and training.

The RRML brings critical laboratory resources and diagnostic surge capability to the doorstep of affected and vulnerable communities, often in hard-to reach remote areas during outbreaks. The UK-PHRST’s microbiology team uses the lab to provide rapid outbreak response, capacity strengthening and research as part of the UK-PHRST’s remit.
Dr Edmund Newman, Director of the UK Public Health Rapid Support Team, said:
"This deployment reflects UKHSA’s commitment to responding rapidly to health threats wherever they emerge and to supporting our international partners in protecting public health globally.
Our teams continue to work closely with all those affected by this outbreak, both in the UK and overseas, to ensure all necessary support is in place. The risk to the general public remains very low."
The UK Public Health Rapid Support Team, academics from the University of São Paulo’s School of Nursing and key Brazilian healthcare stakeholders have co-created, for the first time, gender-based Infection Prevention and Control (IPC) recommendations during disease outbreaks for the Brazilian healthcare context during a research workshop on 10 March 2026. These recommendations aim to significantly improve the safety of patients and healthcare workers in Brazil, especially women, who make up a significant proportion of the workforce, but whose needs are currently under recognised.
The workshop brought together over 20 experts from across Brazil involved in IPC, ranging from the World Health Organization Pan American Health Organization (WHO PAHO), Brazilian Ministry of Health, Ministry for Women, Brazilian Health Regulatory Agency (ANVISA), epidemiologists, regional healthcare professionals and many more.

The workshop is part of the ongoing co-developed research project Influence of gender in the implementation of infection prevention and control (IPC) measures in hospitals in Brazil during outbreak response. Workshop participants drew on the findings from the research project which included results from a literature review, written survey and qualitative interviews with key Brazilian experts. Together, the group discussed and proposed several actionable gender inclusive IPC recommendations for Brazil based on their feasibility. These were then refined and ranked on their ability to be implemented on the ground.
Throughout the study, UK-PHRST’s IPC and Social Science teams have provided technical expertise, supporting Brazilian counterparts undertaking the research.
Maria Clara Padoveze study co-lead from the University of São Paulo School of Nursing said: “Working with the UK-PHRST has allowed us to co-develop a high-quality research project that harnesses both Brazilian and UK expertise and skillsets, particularly regarding gender expertise, in a harmonious and equitable way.”
Based on the project’s findings and rich discussion during the workshop, the next step is a roadmap – developed with support from the UK-PHRST Capacity Strengthening team - outlining how to strengthen gender-equitable IPC policy and practice recommendations for use in Brazil. The team hope to support the production of national policy and practice recommendations that can also be adapted to other similar. low-to-middle income country contexts.
The team’s focus on implementable and multi-disciplinary outputs is clear, with Cat Makison Booth, IPC specialist on the project from the UK-PHRST saying; “We are delighted to have worked with our Brazilian partners to co-create this research project by providing our expertise to help produce findings that are truly cross cutting and relevant for Brazilian health care professionals and patients.”
Sustainability has been central to the project’s approach, thanks to its inclusion of USP nursing students and early career researchers as part of the project team. Julia Harasaki, a USP nursing student who is part of the project team said: “Thanks to this project, in my future career, I want to take forward new ways of implementing IPC measures, thinking about gender, race, social class, to reduce inequalities in healthcare.” The project has even led to the development of a further dedicated PhD project exploring the dynamics of gender in IPC measures during disease outbreaks. This will help the team ensure that their findings will be taken forward through the course of their team member’s own future careers.
If you are interested in learning more about infection prevention and control in practice, consider studying LSHTM's Professional Diploma in Tropical Nursing which is one of the UK’s leading course in global public health nursing.

The UK Public Health Rapid Support Team (UK-PHRST) is proud to be contributing technical expertise to the GOARN Regional Outbreak Response Scenario Programme, launched this week in Trinidad and Tobago in partnership with the Caribbean Public Health Agency (CARPHA), the World Health Organization (WHO) and the Global Outbreak Alert and Response Network (GOARN).
Running from 16-20 March 2026, this five-day, high-intensity simulation exercise brings together 24 public health professionals from CARPHA, WHO Pan American Health Organization (PAHO) and seven Caribbean Member States, spanning disciplines including surveillance, laboratory services, risk communication, logistics, clinical management, and infection prevention and control. UK-PHRST joins a wider GOARN global faculty team that includes technical experts from the United States and European Centres for Disease Prevention and Control (US CDC and ECDC) and the University of Western Australia, Fiocruz Brazil.
The Caribbean presents a distinctive and complex epidemiological landscape. The region's many small, highly interconnected islands, porous borders, heavy dependence on tourism, and exposure to climate-related disasters create conditions in which infectious diseases can spread rapidly and across borders. Recent years have seen the region face outbreaks of measles, dengue, chikungunya, and cholera, alongside increasingly severe hurricane seasons. These realities make the case for a well-trained, coordinated, and regionally connected response workforce – which is what this programme is working to build.
This programme represents the second phase of CARPHA's collaboration with GOARN, building on a Regional Orientation Workshop held in August 2025 and supported by UK-PHRST, which brought together 34 participants to develop core deployment skills. Where that first phase focused on foundational training, this week's exercise moves into operational simulation - placing participants in a realistic, evolving outbreak scenario designed to test their capacity to respond under sustained pressure.
Ed Newman, Director of UK-PHRST, and co-Chair of the GOARN Steering Committee said, “This training brings together some of the best expertise in global public health response, and UK-PHRST is proud to support CARPHA and GOARN in delivering it. Building on the foundational work we supported with CARPHA in August 2025, we are committed to sharing technical expertise with partners across the globe to strengthen outbreak response capacity.
“This exercise demonstrates what sustained international collaboration between the experienced GOARN network partners can achieve - strengthening local, national and regional public health emergency workforces and their regional and international surge capacity.”
Initiatives like this - regionally owned, internationally supported, and grounded in realistic simulation - are the kind of sustained investment that genuinely shifts preparedness. As CARPHA Executive Director Dr. Lisa Indar noted at the Opening Ceremony, "An outbreak can arise with little warning, and the timeliness and effectiveness of our response can determine whether it remains a contained event or escalates into a public health crisis capable of overwhelming national health systems."
GOARN Manager Armand Bejtullahu echoed this, noting that the programme forms part of WHO's efforts to operationalise the Global Health Emergency Corps framework - linking national responders regionally and globally to enable faster, more coordinated responses to public health events.
The programme is funded through CARPHA's Pandemic Fund Project, with CARPHA as the Executing Agency and the Inter-American Development Bank as the Implementing Entity. It forms part of a broader initiative to reduce the public health impact of pandemics across the Caribbean through strengthened surveillance, laboratory systems, and workforce capacity.
V-TARDIS project holds multi-country stakeholder workshop to strengthen detection and surveillance of viruses

UK-PHRST scientists alongside stakeholders from MRC Unit the Gambia at LSHTM, Centre de Recherche et d'Analyse Médicale (CRAM) Guinea, Liverpool School of Tropical Medicine and University of Surrey held a virtual workshop in October as part of the joint research project Toolbox approach for rapid development of methods for detection and surveillance of new, emerging, and re-emerging viruses (V-TARDIS).
The workshop brought together the key study stakeholders to discuss the literature review and survey findings, understand local challenges for virus detection and surveillance and identify priority pathogens across the region.
The research aims to identify what workflows, methods and analysis pipelines would be needed in a flexible diagnostic “toolbox” to strengthen preparedness for future outbreaks.
Researchers deploy the innovative “lab in a suitcase” in Mombasa County as part of feasibility study for portable metagenomics
Mombasa County in Kenya continues to respond to an ongoing mpox outbreak since the country’s first confirmed case in July 2024. Amidst this ongoing outbreak, the UK-PHRST and KEMRI-Wellcome trust RAViG project team deployed its “lab in a suitcase” for the first time in November 2025. The mobile lab helped identify mpox cases by testing skin lesion samples and collecting clinical information from 33 participants.
The on-site lab testing enabled prompt medical care whilst providing critical evidence to help researchers assess the feasibility of using portable sequencing during outbreak response. It is hoped that in-field technologies will reduce the need to transport samples to central laboratories which cost time and resources, ultimately leading to quicker diagnoses and lives saved during outbreaks.
Training Community Health Workers in Zambia

In November 2025, Community Health Workers (CHW) in Zambia completed a Training of Trainers (ToT) course using the Community Health Worker Training Package. The course supports the implementation of enhanced community alert, preparedness, response and resilience capabilities across Zambia.
This builds on UK-PHRST’s ongoing work with Uganda and Ghana to co-develop Community Protection guidance, checklists, curricula and methods for managing disease outbreaks. UK-PHRST supported the design and content of the CHW and National ToT training materials, as well as delivering modules.
Through interactive sessions, demonstrations, group work, case scenarios and role-plays, participants mastered the CHW emergency preparedness and response training modules while practising facilitation skills using adult learning principles and participatory methods. The workshop produced a roadmap for rolling out the training across all regions of Zambia, with clear ownership for monitoring and evaluating.
Training and equipping Monserrat with respiratory protection during outbreaks
Following a capacity strengthening request from the Monserrat Ministry of Health to UKHSA’s UK Overseas Territories (UKOTs) programme, Infection Prevention and Control specialists Janice Toplass and UK-PHRST researcher Cat Makison Booth visited the island to co-develop a sustainable national respiratory protection equipment programme for healthcare workers.
During their visit, Janice and Cat trained local healthcare workers to assess, fit and use respiratory protective equipment securely and safely, ensuring protection from potential airborne pathogen exposure during their work.
In all, they trained 10 healthcare workers to be “fit testers”, collectively completing 110 fit tests and ensured 49 healthcare workers were provided with the correctly fitted respiratory kit – the majority of the workforce on the island. The properly fitted respirators mean that the island’s healthcare workers are protected from infection risk during potential future airborne disease outbreaks.
UK-PHRST support Sierra Leone to strengthen national Mental Health and Psychosocial Support offering
UK-PHRST Mental Health and Psychosocial Support (MHPSS) expert Dr Biksegn Yirdaw supported Sierra Leone’s National Public Health Agency (NPHA) during a one-month placement in October 2025, strengthening national MHPSS capacity during the mpox outbreak.
Working closely with NPHA colleagues, Dr Yirdaw focused on strengthening MHPSS coordination mechanisms, developing a strategic national MHPSS emergency response plan, and delivering MHPSS training workshops to local healthcare workers.
Dr Yirdaw also provided strategic support to NPHI colleagues as part of their ongoing national MHPSS strengthening programme. Dr Yirdaw contributed to the development of an MHPSS gap assessment tool to identify gaps in existing mental health support availability and help co-ordinate comprehensive care for vulnerable groups. The NPHA also successfully launched the National Multisectoral MHPSS Provider Program Guidelines for 2025-2030 during Dr Yirdaw’s placement, providing a framework for coordinated, tailored and quality MHPSS services during emergencies.

Dr Nadine Beckmann, UK-PHRST’s Social Science team lead featured as a panellist at LSHTM’s recent Health Misinformation: UNPACKED event. The event sought to share knowledge and inspiring ideas about how to respond to high-level health misinformation spreading in the media, on social, and online.
Nadine spoke about what it’s like to deal with misinformation and rumours in a disease outbreak context, drawing extensively on her deployment experience and her team's research in Sierra Leone and Tanzania to track rumours and concerns about COVID-19. This study aimed to better understand the relative influence and mechanisms of online and offline COVID-19 rumours and identify solutions to address community concerns during health emergencies.
The event included many other misinformation experts from LSHTM and other universities, the media, NGOs, and government.
UK-PHRST and Ugandan partners strengthen mental health support during disease outbreaks through national framework drafting and simulation-based training
In September, the UK-PHRST Mental Health and Psychosocial Support and Capacity Strengthening teams, working alongside the Ugandan Ministry of Health and Makarere University, delivered an in-person workshop aimed at strengthening the outbreak preparedness and mental health response capacities in Uganda.
The workshop built on the previous collaboration between UK-PHRST and Ugandan partners through the joint research project Making mental health and psychosocial support (MHPSS) part of outbreak planning in Uganda. Attendees included staff from the Ugandan Ministry of Health and outbreak response co-ordinators from the Ugandan Incident Management System and MHPSS Technical Working Group.
Across the five-day workshop, UK-PHRST and Uganda Ministry of Health shared learned lessons from the joint research project, worked together to draft a national MHPSS plan and conducted a tabletop exercise covering key MHPSS skills for the national outbreak response team.
UK-PHRST co-design and delivers regional workshops on MHPSS with Africa CDC in the Northern African Region
In September, UK-PHRST co-designed and delivered a five-day Mental Health and Psychosocial Support (MHPSS) training simulation workshop in Cairo, Egypt, focused on strengthening outbreak preparedness and response in Northern Africa. The workshop aimed to enhance the integration of MHPSS into emergency preparedness and response plans.
The simulation exercise was concluded with a half-day research writing skills workshop to improve learning and the use of evidence related to MHPSS in emergency preparedness and response efforts. Additionally, UK-PHRST supported the training of a new cohort of MHPSS experts who will join the African Volunteer Health Corps (AVoHC) roster and will be able to provide support to Countries in Northern Africa to strengthen their MHPSS preparedness and response.
Over 20 participants attended both workshops from Northern African countries.
UK-PHRST Microbiologists help KEMRI-Wellcome Trust scientists prepare to deploy portable lab in Kenya

In July 2025, members of UK-PHRST’s microbiology visited the KEMRI-Wellcome Trust Research Programme in Mombasa to conduct a hospital clinical dry run with portable lab equipment as part of the Rapid virus genomics for outbreak investigation (RaViG) research study. This follows a previous visit in March to test viral sample collection and analysis.
The success of the laboratory readiness assessment now means the Kenyan team are ready to deploy the portable lab in the field to collect samples as part of the research study which aims to assess the feasibility of using portable sequencing during outbreak response.
Read more about the research project.
Guardians of Health - Community Leaders Event Based Surveillance research project supports Cabo Verde response during recent floods
The early warning system app produced as part of the joint UK-PHRST and ProEpi Guardians of Health - Community Leaders Event Based Surveillance research project was recently adapted to help support the Cabo Verdean local government response to flooding in São Vicente.
Led by the team in Cabo Verde and Brazil, the app was quickly adapted, incorporating new variables and features that allow monitoring the impacts of the disaster, identifying cases of disease, and supporting public health actions.
With health services overwhelmed after the disaster, the Health Guardians strategy established itself as a strategic ally in preventing secondary outbreaks, supporting case triage, and providing reliable information to authorities.
Read more about this story.
UK-PHRST and MRC/UVRI & LSHTM Uganda Research Unit hold community, regional and national workshops to deepen understand of Rift Valley Fever in Uganda

In September 2025, UK-PHRST’s social science team worked with researchers from the Medical Research Council /Uganda Virus Research Institute & London School of Hygiene and Tropical Medicine Uganda Research Unit to hold three workshops at the community/sub-county, district and national levels to gather views and input on the findings of their co-led research study: ‘A participatory study to identify gaps and solutions to zoonotic disease detection and reporting: a case study of Rift Valley Fever in Kalungu District, Uganda’
The research study is exploring the gaps in detection and reporting of Rift Valley Fever in Uganda. Using RVF as a case study, the research aims to strengthen the prevention and detection of infectious diseases nationally.
Attendees across the three workshops included representatives from Kyamulibwa and Lwabenge sub counties, veterinary officers, health inspectors, community leaders, community advisory board members and representatives from Ugandan Ministries of Agriculture, Health, Water and Environment and the Uganda Virus Research Institute.
Each workshop included interactive presentations covering the study’s aims, methods and key findings, discussions of the study implications given local experiences and collaborative sessions with attendees to co-develop recommendations. The workshops aimed to validate the study findings and gain a deeper understanding of local perspectives and identifying barriers and opportunities for improving detection and reporting of zoonotic diseases in Uganda.
The researchers are now working collaboratively with the different stakeholders to co-develop reports and roadmaps outlining practical and policy recommendations to improve zoonotic disease detection and reporting in Kalungu District and ultimately inform national strategies for similar settings across Uganda.
Disability mainstreaming in the Kenyan public health system: Addressing equity during outbreak response – stakeholder workshop

UK-PHRST joined the African Institute for Health & Development, the Kenyan National Public Health Institute and other partners at the first stakeholder meeting to discuss their new joint research project aiming to improve disability inclusion in public health emergency preparedness and response in Kenya.
The research study will focus on two main questions:
- What are the needs of people with disabilities during a typical outbreak response in Kenya? Have their needs been met during past outbreak responses
- How can we maximise the benefit of disease prevention and control measures and reduce the potential to cause unintended harm for people with disabilities during outbreak response in Kenya?
To gather insights, the research team will conduct interviews and focus groups with people with disabilities, caregivers, responders, and policymakers. Alongside this, the research team will undertake a scoping review of global literature on the group’s experiences during disease outbreaks and review existing data and documents on past outbreak responses.
Ultimately, the researchers hope that by pinpointing the needs of people with disabilities during disease outbreak and identifying gaps in Kenya’s current health emergency response system, they will develop a plan for improving the reach and reducing the unintended harm of outbreak response measures for people with disabilities across Kenya.
The UK Public Health Rapid Support Team, working alongside the Global Outbreak and Response Network (GOARN), has successfully delivered the GOARN Tier 1.5 Orientation to National and International Outbreak Response Workshop for the first time.
In collaboration with the Caribbean Public Health Agency (CARPHA), 34 public health professionals including CARPHA personnel based in Trinidad and Tobago and representatives spanning 10 Member States took part in the training. Attendees included emergency response focal points from ministries of health, public health surveillance officers, laboratory professionals, and specialists in risk communication and One Health - marking a significant step forward in strengthening the region’s capacity to respond rapidly and effectively to public health emergencies.
The three-day event - consisting of two outbreak response workshops back-to-back – involved classroom-based training using scenarios, case studies, presentations and discussions followed by an evaluation workshop of CARPHA’s response plans and mechanisms.
These intensive workshops were designed to help close identified gaps in the region’s emergency response architecture, particularly in relation to the deployable response workforce, internal operational processes, and multisectoral coordination mechanisms. The response plan review then examined CARPHA’s capacity and capability to respond, using relevant scenarios to stress test existing plans and procedures, clarify roles and decision-making arrangements, and identify practical improvements in multisectoral coordination.
UK-PHRST was able to deliver this workshop through a carefully selected team of facilitators who themselves recently completed the GOARN Tier 1.5 training. The UK-PHRST team combines extensive GOARN and WHO field experience with proven adult learning expertise and includes former deployees who provide authentic insights into the realities, challenges, and rewards of international outbreak response work.
Dr Ed Newman, Director of UK-PHRST and Co-Deputy Chair of the GOARN Steering Committee, noted the lasting value of the programme:
“We’re delighted to partner with CARPHA on this initiative in support of their vision to expand regional Public Health Emergency Response capacity and capability. Working alongside GOARN, we’re proud that UK-PHRST has the expertise to deliver these workshops, sharing our learning and experience and that of our partners - helping ensure CARPHA and its Member States are better equipped to respond to future public health emergencies. This partnership demonstrates the power of international collaboration in building resilient public health response systems and reflects our shared commitment to strengthening global health security.”

Dr. Lisa Indar, Executive Director of CARPHA, praised the collaborative effort and its impact:
“These workshops strengthen our collective readiness to face the next public health emergency. By enhancing the skills of our regional deployers and testing our coordination protocols under realistic conditions, we are ensuring that CARPHA and its Member States can respond quickly and decisively when outbreaks occur. Our continued priority is the safeguarding of lives and protection of our livelihoods.”
British High Commissioner to Trinidad and Tobago, H.E. Jon Dean added “The UK is proud to have supported this important initiative through the UK Public Health Rapid Support Team, in close partnership with CARPHA and WHO GOARN. The training represents a meaningful step toward strengthening the speed and effectiveness of public health emergency responses in Trinidad and Tobago and across the Caribbean. This collaboration reflects the UK’s enduring commitment to regional cooperation, resilience, and shared learning with the Caribbean"
The knowledge and skills gained during the workshops will now be integrated into national public health systems, expanding the region’s pool of professionals who are trained, tested, and ready for rapid deployment. By building a skilled and responsive health emergency workforce and testing coordination protocols under realistic conditions, this initiative is supporting the long-term sustainability of emergency preparedness in the region.

Joint UK-PHRST and Africa CDC research study confirms vital role international deployments play in Africa’s outbreak response

A new study jointly carried out by the Africa Centres for Disease Control and Prevention (Africa CDC) and UK-PHRST highlights the critical role international health teams play in strengthening outbreak response across the African continent. The study also highlights the need for more strategic and locally tailored support models to ensure long-term sustainability and effectiveness.
Study participants recently gathered with representatives of international and regional public health bodies to review and validate these findings. Together, they moved beyond the academic findings and developed series of recommendations to put the findings into practice. The partnership hopes to create a good practice guide and roadmap for transforming short term deployment gains into long-term sustainable solutions in outbreak management. This represents a significant step forward in moving from individual deployment experiences to systematic, evidence-based approaches that can benefit everyone.
Dr Femi Nzegwu, Assistant Professor at the London School of Hygiene & Tropical Medicine and Monitoring, Evaluation and Learning lead at UK-PHRST, said: “Evidence-informed learning must guide how we improve emergency public health deployments. The findings of the report validate experiences across Africa but also point to what must change to ensure deployments are more effective, context-specific, equitable, and empowering for Member States.”
Read more about this latest update
Guardians of Health Project - Community Leaders researchers share findings at leading conferences in Cabo Verde and Sweden
Throughout June, the ProEpi team, part of the UK-PHRST collaborative research Guardians of Health - Community Leaders Event Based Surveillance study shared the research project’s progress and initial findings at several conferences.
Between 22 and 27 June 2025, the project’s technology professional Rogério Carminé represented the study team at the Human-Computer Interaction (HCI) 2025 International Conference in Sweden. The event brought together experts, researchers and professionals from various countries to debate the latest advances in digital technologies, with a focus on human-centred solutions.
Dr Carminé presented the development of the mobile application and its implementation in Brazil and Cabo Verde, and addressed the cross-cultural dimension of the project and the challenges of implementation in different contexts. The presentation was well-received, generating enthusiasm for its participatory approaches and the potential for impact in other developing countries.
Similarly, on 24 and 25 June 2025, members of the project in Cabo Verde presented the project at the 2nd Scientific Meeting of Field Epidemiology in Cabo Verde, a leading event for the country’s field of public health. The conference brought together local health managers and international consultants as well as graduates of the Cabo Verde field epidemiology training project. The conference allowed study researchers to highlight the joint study’s findings to the Cabo Verdean scientific community and decision-makers.
UK-PHRST prepares deployees through new peer-learning approach and launches dedicated resource hub for shared learning
UK-PHRST recently held the latest iteration of its deployment training programme; ‘The Deployment Peer Learning Programme (DPLP)’ and launched a new resource hub on the Global Health Network aimed at enhancing the knowledge, skills and confidence of UK-PHRST deployees and partners to effectively engage in outbreak response activities.
This year’s training programme capitalised on UK-PHRST and partners' collective deployment experience by taking a peer-learning approach, where new and experienced deployees learned from one another. The training followed a blended learning design consisting of online sessions and a three day in-person event. 26 participants attended including UK-PHRST staff, UK-PHRST reservists, Field Epidemiology Training Programme fellows and partner organisations including Africa CDC and World Health Organization Regional Office for Africa (AFRO).
Further, as part of our commitiment to supporting the sustainable long-term impact of our activities, UK-PHRST has developed and launched a new dedicated resource hub. Drawing on the work with our partners across our triple remit of deployments, capacity strengthening and research, the resource hub is a place to share freely-accessible, co-developed, evidence based tools and guidance for anyone looking to enhance their knowledge and skills to effectively engage in outbreak response activities.
The new hub represents UK-PHRST's commitment to knowledge sharing and collaborative learning, enabling public health professionals globally to access the insights and practical guidance developed through our extensive partnership working and experiences. The resource hub will be continuously updated with new materials and insights as they are developed, ensuring access to the most current guidance available.
Reflecting on the training, Tanu Soni, UK-PHRST Capacity Strengthening Officer and Deployment Training Co-Facilitator said: “I am glad that this year’s peer-learning programme embraces the complexities of public health emergencies — such as politics, power struggles, and emotional responses and addresses this complexity through experiential learning, with an emphasis on soft skills and knowledge sharing. Participants will also have the chance to further explore these dimensions through our new Global Health Network online resources hub.”
Find out more about this project.
Biosafety training for mobile genomics laboratory deployment in coastal Kenya

In June, UK-PHRST’s microbiology team developed and delivered training to staff at the KEMRI-Wellcome trust in mobile genomics lab biosafety protocols as part of the ongoing Rapid virus genomics for outbreak investigation (RaViG) study in Kenya.
The five-day training consisted of theoretical approaches to handling, biosafety and sample processing followed by independent team-based exercises simulating outbreak sample processing, decontamination, PPE selection, waste handling, and incident response protocols. Finally, the participants reviewed their performance and key lessons learnt.
The training, delivered alongside UKHSA’s Novel and Dangerous Pathogens Training Team, aimed to enshrine sustainability and long-term capacity building by strengthening biosafety and outbreak response capacity within KEMRI and Kilifi County Hospital, ultimately enhancing their ability to independently respond to outbreaks in the future.
UK-PHRST support epidemiological training in outbreaks and surveillance for regional epidemiologists in Ukraine

In June, UK-PHRST supported the planning and development of materials for an epidemiology training course in surveillance, outbreak detection and data analysis for regional epidemiologists affiliated with the Ukraine Public Health Center of the Ministry of Health.
The in-person event was led by LSHTM academics and took place in close collaboration with the Public Health Centre of the Ministry of Health of Ukraine and WHO Ukraine. The training aimed to increase participant’s general epidemiological knowledge and technical skills and help them apply this knowledge at the regional level across Ukraine to improve the country’s already established surveillance and early warning systems.

The training focused on delivering practical, high quality and up-to-date material during an ongoing conflict. 25 attendees worked in small groups to discuss specific scenarios and practice applying the local lens of Ukraine’s public health system to monitoring for routine concerns of new outbreaks of vaccine-preventable diseases like measles and West Nile virus.
EPI-WIN webinar: empowering Community Health Workers (CHWs) through capacity strengthening for outbreak detection and response
UK-PHRST’s Head of Capacity Strengthening Dr Claire Bayntun presented at a WHO webinar in April discussing lessons from the UK-PHRST’s work to empower community health workers through capacity strengthening initiatives in outbreak detection and response.
During her presentation, Claire advocated for the importance of community health workers in successful outbreak management. She also highlighted the benefits of a “community protection” centred approach to outbreak response by showcasing her team’s recent collaboration with WHO HQ and AFRO. Together, they delivered a multidisciplinary package of support to Ugandan community health workers during the Ebola outbreak in February 2025.
See the full recording.
UK-PHRST visit Cabo Verdean National Public Health Institute as part of Guardians of Health research project
In February, UK-PHRST team members and project collaborators from University of Brasilia and ProEpi, Brazil, visited the National Institute of Public Health of Cape Verde (INSP) as part of the Guardians of Health - Community Leaders Event Based Surveillance UK-PHRST research study.

The team participated in a community leader training workshop, met with national partners at the National Public Health Institute and presented preliminary project data to community leaders participating in project health surveillance. Meetings also took place with project focal points of the Guardians of Health project, across nine municipalities of the island of Santiago, who have been instrumental in community leader recruitment and project delivery.

As part of the visit, UK-PHRST’s Deputy Director for Research, Professor Gwenda Hughes was interviewed by Cabo Verdean news outlets, including Jornal da Noite on Radiotelevisão Caboverdiana.
Dr Maria da Luz Lima, President of the INSP, explained the national importance of the research and visit: “We are monitoring to see the results and if we have good results we will make a proposal to the central services of the Ministry of Health to explore implementing this event-based surveillance project”.
Subject to the results of the pilot study, the project team hope to roll out the new surveillance system in both Brazil and Cabo Verde.
Testing mental health preparedness and response in Uganda

In March, as part of the UK-PHRST research project Making mental health support part of outbreak planning in Uganda, the Ugandan Ministry of Health, with design and delivery support from the UK-PHRST’s Capacity Strengthening and Research teams, organised a tabletop exercise to assess MHPSS interventions in Uganda. The exercise brought together stakeholders from the Ministry of Health and district health teams from Bundibugyo and Kasese districts.
The team used a tabletop exercise to simulate outbreak scenarios that might happen in real life, allowing stakeholders to work through what their response might be.
The tabletop exercise in Uganda both assessed the Mental Health and Psychosocial Support (MHPSS) preparedness and response status at the national and district levels and acted as a learning exercise by highlighting gaps in current response capacity. The exercise brought out practical lessons and recommendations to improve response in future disease outbreaks.
Read more about the exercise and the MHPSS Uganda project.
Trialling virus sample collection and testing with KEMRI-Wellcome Trust

In March 2025, members of the UK-PHRST’s microbiology and evaluation teams visited the KEMRI-Wellcome Trust Research Programme in Kilifi to carry out a test run of viral sample collection and analysis with Kenyan partners as part of the Rapid virus genomics for outbreak investigation (RaViG) research study.
The activity aimed to practice and evaluate sample inactivation, safety and equipment setup. It also gave the study team hands-on experience with portable genomics to prepare for sample collection and in-field diagnostics to assess the feasibility of using portable sequencing during outbreak response.

As part of the visit, the team also convened the project’s Steering Committee in Nairobi with representatives from the study team, the Ministry of Health, Kenya and public health officers from Kilifi, Kwale, Taita-Taveta, Tana-River, Lamu and Mombasa.
Read more about the research project.
UK-PHRST and World Health Organization support Uganda to tackle infectious disease outbreaks

A joint training session in February 2025 aimed to strengthen Uganda’s Ebola response in the midst of an outbreak, and enhance the country’s ability to prevent, detect, and respond to health emergencies.
The UK-PHRST collaborated with the WHO Uganda country office, WHO AFRO and Community Readiness and Resilience unit of WHO Headquarters, the Ministry of Health Uganda and others to conduct the training on Ebola disease detection and management for community health workers from Kole, Wakiso and Mukono districts.
Africa CDC holds Africa Volunteer Health Corps induction event
In March, Dr Claire Bayntun, UK-PHRST Head of Capacity Strengthening, attended an African Volunteers Health Corps (AVoHC) induction event where 120 rapid responders gathered at Africa CDC headquarters for a five-day induction course into the network.
AVoHC was first launched in 2015 to deal with the ongoing Ebola outbreak affecting Guinea, Liberia, and Sierra Leone at the time.
Africa CDC, working with partners including UK-PHRST, designed and developed the AVoHC induction course to address the skills gap and ensure all AVoHC members are fully prepared for efficient and effective deployment during a health crisis.
UK-PHRST has helped Africa CDC develop the training materials for AVoHC including the general curriculum, facilitator’s manual, facilitator training and a specific mental health training package. Dr Claire Bayntun, UK-PHRST Head of Capacity Strengthening attended the induction event on behalf of the UK-PHRST and said: “We are proud to have worked alongside Africa CDC on AVoHC since its inception. This is one of the most valuable assets that Africa CDC has offered to the African continent to support outbreaks and we look forward to seeing what AVoHC will do in the future.”
Since its launch, 274 AVoHC members have successfully completed the training, equipped with the critical skills and knowledge needed to contribute to public health emergencies and strengthen response efforts throughout the continent. Following the successful recruitment of 385 epidemiologists from various Member States across the continent, Africa CDC plans to accelerate the rollout of the AVoHC induction course in 2025.
Read more about the AvoHC programme.
UK-PHRST MHPSS team help host academic writing training in Addis Ababa

In January, the UK-PHRST’s Mental Health and Psychosocial Support (MHPSS) team partnered with ARQ International and Intervention Journal to organise an academic writing training course for MHPSS experts.
The training taught participants to enhance their skills and understanding of academic writing. They engaged in theoretical presentations, interactive exercises and focused writing time, covering essential topics such as how to formulate a working title, pitch an academic idea, draft an outline, navigate academic publishing, use AI, and set writing goals. The training is being followed by ongoing mentorship of the participants, by linking them with experienced researchers, and providing several additional online capacity strengthening sessions.
Ultimately the training aims to help bridge the gap between MHPSS practice and research, ensuring that practitioners can use research writing as a powerful tool to amplify local voices and strengthen evidence-based practices within MHPSS.
Another in-person session and follow-up mentorship with a new cohort of front-line MHPSS leaders is planned for the up-coming meeting of the MHPSS Surge Support Mechanism.
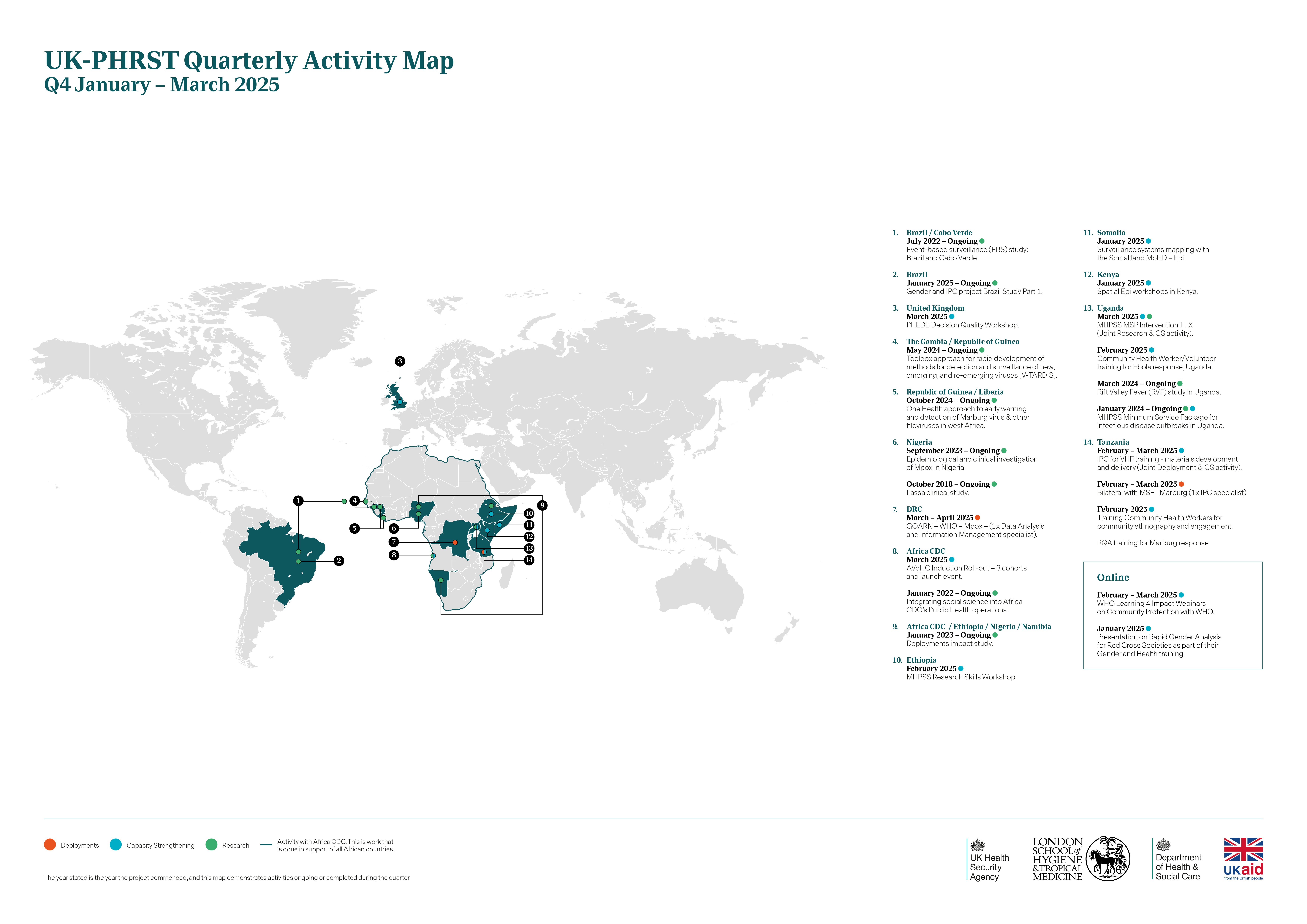
View our quarterly map to see our activities between January and March 2025.
The UK-PHRST showcased its expertise in outbreak response on multiple fronts at the UKHSA Conference in Manchester, from hosting a panel including international players in disease outbreak response, to sharing learnings from our deployment experiences.
The UK-PHRST organised panel featured leading voices in global response efforts and included representatives from the Africa Centres for Disease Control (Africa CDC), the World Health Organization (WHO), Médecins Sans Frontières (MSF), European Centres for Disease Control (ECDC), UK Government Foreign, Commonwealth and Development Office (FCDO) and UK-PHRST.
Chaired by the UK’s Deputy Chief Medical Officer, Dr Thomas Waite, the panel discussed the importance of sustainability in global emergency response for high-consequence infectious disease outbreaks of international concern. Focusing particularly on low- and middle-income countries, the group held active discussions on the current models of outbreak response, cooperation and collaboration, and the impact, risks and opportunities in relation to recent changes in the donor policy landscape.

Key emerging themes included the effectiveness of response, how we support nationally-led responses as international partners, and the and the importance of partner coordination and equity for sustainable outcomes. Panelists also reflected on the the successes and challenges of innovations in technology as well as the importance of community-centred responses.
Ed Newman, UK-PHRST Director said:
“We are delighted to have hosted many of our valued international partners as part of the UKHSA conference in Manchester. These discussions have reinforced the importance of partnership and sustainability in making impact before, during and after disease outbreaks, something the UK-PHRST is proud to actively champion.
“We cannot rest on our laurels however, we must continue to further support partners with their national response to public health emergencies. Strengthening capacity and knowledge outside of response operations to ensure readiness to respond, through co-development and co-creation with our valued international partners is key to safeguard global and UK health security.”
Separately, UK-PHRST’s Epidemiology co-Lead and core deployee Dr Victor Del Rio Vilas, spoke during a session showcasing UKHSA’s work around the world to enhance global health security through its strategic goals to ‘prepare, respond, and build’. Victor outlined the UK-PHRST’s role of responding rapidly and at short notice to requests from national governments and multinational global health partners to support the prevention and control of infectious disease outbreaks, before they develop into global emergencies. He shared the experience, reflections and learnings from his 2024 deployment alongside to South Sudan with the Global Outbreak Alert and Response Network where he provided epidemiological support to in-country partners alongside UK-PHRST Field Epidemiologist Tina Sorensen.
About UKHSA conference
The 2025 UKHSA Conference is a distinctive gathering of up to 3,000 colleagues, experts, partners and stakeholders over two days; as we work to deliver our mission of preventing and responding to health threats, saving lives and protecting livelihoods. The conference programme explored the latest advancements, strategies and innovations in health protection and demonstrate the unique impact of UKHSA through our scientific, academic and commercial offer, and the power of our collective endeavour through partnership. The conference welcomed colleagues from across the life sciences landscape, industry partners, professionals within health protection and public health in local government, international partners, the NHS and community and charity organisations.
Evolving landscapes: The future of sustainable global response to public health emergencies and outbreaks
- Professor Yap Boum II, Deputy Incident Manager for the Continental Mpox response, Africa CDC
- Dr Thomas Hoffmann - Head of Emergency Preparedness and Response, ECDC,
- Dr Olivier Le Polain - Unit Head, Epidemiology and Analytics for Response Unit, WHO Health Emergencies Programme
- Dr Melissa McRae - Senior Researcher in Medical Ethics, MSF
- Uzoamaka Gilpin – Africa Global Health Security Team Leader and Senior Responsible Officer, Tackling Deadly Diseases in Africa Programme Phase II (TDDAP 2) , Foreign, Commonwealth and Development Office (FCDO)
- Dr Edmund Newman, UK-PHRST Director
- Dr Thomas Waite - Deputy Chief Medical Officer, Department of Health and Social Care (DHSC) - session Chair
UKHSA around the world: Working with partners to prepare, respond and build
- Dr Victor del Rio Vilas - Senior Epidemiologist, UK-Public Health Rapid Support Team, UKHSA
- Dr Olúṣọlá Aruna - Country Lead/Senior Public Health Advisor, International Health Regulations (IHR) Strengthening Project, UKHSA
- Dr Haydn Cole - Group Leader, Chemicals and Poisons, UKHSA
- Anna Wechsberg - International Director and Director for EU, Trade and the Union, DHSC - session Chair
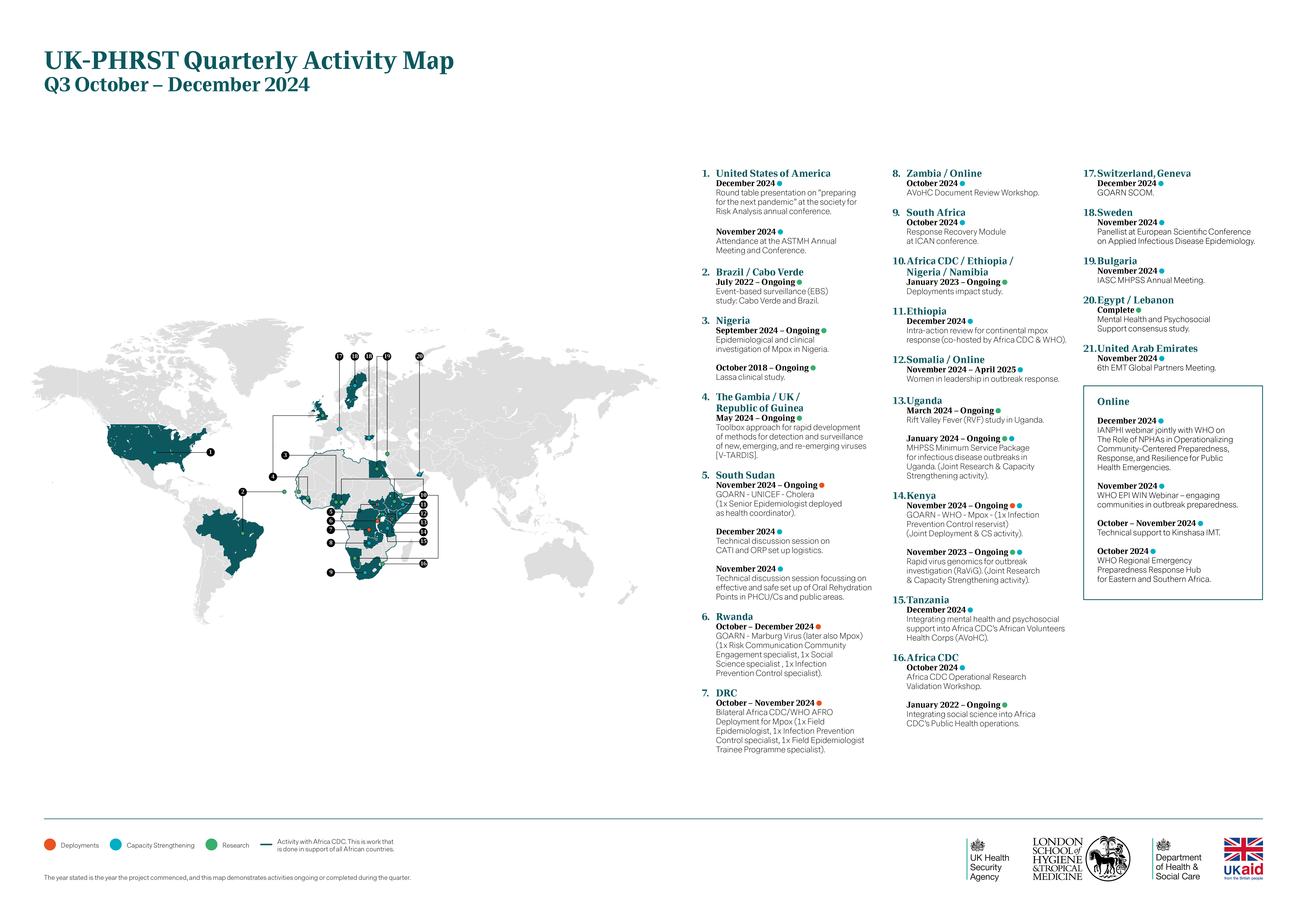
View our quarterly map to see our activities between October and December 2024.
The UK-PHRST team has been busy delivering capacity strengthening activities, advancing partnerships and contributing to the global discourse around outbreak response. Highlights below:
Gender in Emergencies Group – Rapid Gender Analysis Mpox Outbreak in DRC Report
UK-PHRST’s Social Equity & Human Rights Officer, Olive Leonard was recently involved in researching and drafting the first gender analysis on the impact of mpox in the Democratic Republic of the Congo and neighbouring countries, in collaboration with the Gender in Emergencies Group.
The analysis highlights key findings around the challenges that individuals, particularly children, women, and marginalised groups, have faced during the first wave of the mpox outbreak. Alongside its recommendations, researchers call for a gender-responsive and intersectional approach to be taken on the ground. The hope is that the report will inform public health experts during the next phase of the mpox response in the DRC as the outbreak continues.
Read the full findings and recommendations
Making mental health an integral part of the African Volunteers Health Corps response

In December 2024, Africa CDC and the mental health and psychosocial support team of the UK-PHRST co-led training for the new cohort of 19 MHPSS experts in Dar Es Salaam. During a busy week, the team used interactive scenario-based training to facilitate peer learning among the diverse range of participants, including psychiatrists, psychologists, nurses and social workers.
The training forms part of Africa CDC’s work to respond to public health emergencies across African member states which it is now further strengthening by including mental health and psychosocial support via AVoHC’s work. As a result, the group are now ready for deployment and will continue to receive support from the mental health team through a newly established network.
This training is part of UK-PHRST’s wider work alongside AVoHC and the mental health team at Africa CDC to develop a comprehensive approach to incorporating wellbeing in their range of expertise offered to member states.
Thanks to this work, all AVoHC members, as part of their core training prior to deployment now have essential skills for supporting wellbeing among the people they see in their work, as well as guidance on protecting their own mental health. In addition, systems have been put in place to support wellbeing of the deployed personnel, and leaders have committed to ensuring this remains a key consideration.
Africa CDC has also recruited a new team of mental health specialists to be deployed alongside AVoHC colleagues in the event of future emergencies. This is the first time that this expertise has been made available as part of wider teams addressing IPC, WASH, labs, epidemiology - ensuring response is addressing a full range of required expertise.
UK-PHRST experts support World Health Organization develop Community Health Worker mpox training
UK-PHRST experts recently provided guidance and feedback to World Health Organization colleagues to develop a training package for community health workers and volunteers to enhance their knowledge and skills in mpox community detection and response which could be used in affected countries.
The training aimed to develop a standard training package adapted from existing WHO resources which can be tailored to specific country community-level contexts. Topics covered included early detection, warning, referral and care for mpox.
Communities in the Democratic Republic of the Congo have already started to receive the benefits of the training, as under WHO guidance, national-level trainers delivered a workshop to community health workers and members as part of the ongoing mpox outbreak response activities.
The UK-PHRST team and partners are currently delivering nine research projects. In this edition, read about the first community leader training in Brazil as part of the Community Leaders Event Based Surveillance study and Mental Health and Psychosocial Support implementation workshops in Uganda.
Ongoing research projects
Community Leaders Event Based Surveillance study - First community leader training workshop in Brazil
Throughout the autumn, the Brazilian team partnering on the Community Leaders Event Based Surveillance study began the implementation phase of the Community-Based Event-Based Surveillance (VBE Comunitária) tool by holding the first community leader training workshops in Brazil.
Using the skills learnt during the workshops, local leaders can now report disease outbreaks in the Guardians of Health app. These reports are then analysed by trained health professionals. The project team are aiming to hold another user workshop in the Federal District for the administrative regions of Paranoá and Itapoã, in addition to analysing data for scientific outputs from the study.
Mental Health and Psychosocial Support project team hold implementation workshops in Uganda

Working closely with researchers based at Makerere University, the Ministry of Health in Uganda and Africa CDC, this study aims to use the Mental Health and Psychosocial Support Minimum Service Package (MHPSS MSP) to develop, implement and evaluate a suite of tailored MHPSS interventions that could be used to support outbreak preparedness and response in Uganda.
A series of implementation activities for the MHPSS Uganda project took place in Bundibugyo, Uganda, including orientation of the district team and frontline workers, a workshop for adaptation of MHPSS orientation materials and awareness messages and MHPSS training for healthcare workers.

Dr Ed Newman, Director of the UK Public Health Rapid Support Team (UK-PHRST) has recently been elected as co-deputy chair of the Global Outbreak Alert and Response Network (GOARN) Steering Committee. Dr Mohannad Al-Nsour, Eastern Mediterranean Public Health Network (EMPHNET) was appointed as Chair, with Ed, alongside Dr Daniela Garone, Médecins Sans Frontieres (MSF) elected as co-deputy chairs.
Under the new leadership, the Steering Committee and GOARN partners will continue advancing health security, strategic partnerships and communication, and strengthening the emergency public health workforce capacity.
In this interview, Ed explains more about GOARN, what his new role will entail and UK-PHRST’s involvement in the network.
What is GOARN and why is UK-PHRST involved?
GOARN is a network of over 310 global technical institutions and organisations that respond to acute public health events with the deployment of staff and resources to affected countries. The network delivers rapid and effective support to prevent and control infectious diseases outbreaks and public health emergencies when requested.
UK-PHRST is a GOARN network partner and regularly deploys to outbreaks of infectious disease in response to requests for assistance made by low- and middle-income countries. I’m really proud that UK-PHRST is one of GOARN’s most active deployment partners, meaning we’ve responded to more requests for assistance from GOARN in the last year or two than most other partners in the network.
What does a typical deployment through GOARN look like?
Typically, GOARN will request technical assistance from its network on behalf of a partner who are supporting the national response to an infectious disease outbreak or other public health emergency, such as WHO or UNICEF. This will be a request for assistance in a particular public health discipline such as epidemiology, community engagement, infection prevention and control etc. or for an emergency coordination role such as incident manager, or health coordinator. Where it can, UK-PHRST puts forward offers of assistance to meet the needs of the request. If our offers are selected, we then deploy our experts to join the requesting GOARN partner’s in-country team. This often means being involved in technical advice and coordination at a national level for WHO or UNICEF, whilst working closely with the host country's government on their response. But deployments vary in nature and can involve working within a country office or incident management team in the capital city, to visiting local communities and health centres affected by the outbreak. Typically, we deploy between one to four experts, and deployments usually last for around six to 10 weeks.
What will your role as co-deputy chair of the GOARN Steering Committee involve?
I will form part of the Senior Leadership Team of GOARN alongside my co-deputy chair, and the chair. We will work with other members of the steering committee and the WHO’s GOARN Operational Support Team to ensure GOARN delivers its remit of providing public health response workforce and strengthening national response. We also represent the GOARN Steering Committee and its 300+ partners within the WHO’s Health Emergencies Programme and the wider evolving global health response architecture, as well as at key international meetings where we advocate for GOARN as a network and the important work all its partners contribute to in improving global health security.
Why is this important and what opportunities are there for UK-PHRST?
The Global Health response architecture is going through a period of change with the formation of initiatives such as the Global Health Emergency Corps bringing networks such as GOARN, the Emergency Medical Teams initiative, International Association of National Public Health Institutes (IANPHI), and others together. At the same time, the emphasis on improving readiness to respond to public health emergencies is quite rightly focusing on local and national capacities. During this time of change it is essential that GOARN has strong leadership to ensure the network does its part and maintains its international reputation as a leader in public health emergency response and coordination.
For the UK Public Health Rapid Support Team, this gives us an opportunity to build on our strong reputation in this area and increase our influence on the global stage, further securing our status as key partners in global health security.
What are you most excited for as Co-Deputy Chair?
I am passionate about the power of the GOARN network having first deployed through GOARN in 2012 as a scientist for the UK’s Health Protection Agency, where I supported Uganda’s response to an outbreak of Marburg. I also completed several deployments during the West Africa Ebola outbreak.
I’m excited and privileged to be able to represent this great network and its amazing partners, ensuing it stays at the forefront of global public health emergency response. The level of collaboration and humility within the GOARN partners is inspirational and it is a great team to be part of – where you are constantly reminded of the difference to the lives of those affected by infectious disease outbreaks in some of the most challenging settings in the world.
The UK-PHRST team has been busy delivering capacity strengthening activities, advancing partnerships and contributing to the global discourse around outbreak response. Highlights below:
Supporting Mental Health and Psychosocial Support preparedness to public health emergencies in Africa

The UK-PHRST’s Mental Health and Psychosocial Support (MHPSS) team has been working with the African Public Mental Health Consortium to strengthen public mental health in Africa and deepen the integration of MHPSS into increasingly frequent public health emergencies across the continent.
As part of this work, in collaboration with Africa CDC, the UK-PHRST MHPSS team organised a regional stakeholder workshop in Namibia in September which was attended by emergency preparedness and response (EPR) and MHPSS focal persons representing nine southern African countries. Partners from the WHO, UNICEF and regional NGOs also participated.
The workshop aimed to help the countries develop a comprehensive roadmap of how MHPSS integration would happen in the short, medium and long-term to contribute to the overall goal of strengthening mental health systems for emergency response in the southern Africa region. There was a particular focus on mpox preparedness and response due to the current epidemic.
To make action in this area a reality, the next phase of this work will be to support the countries who have committed to integration of MHPSS into these plans, so that we are able to attend to the comprehensive needs of populations during emergencies.
Technical case study: Conducting cross-border Risk Communication and Community Engagement scenario-based training

The UK-PHRST is pleased to share a technical case study describing the successful collaborative delivery of the first-of-its-kind cross-border RCCE training to the Ministry of Health, Red Cross/Crescent National Society, UNICEF and WHO staff from seven East African countries - Kenya, Somalia, Ethiopia, South Sudan, Uganda, Rwanda, and Tanzania.
The case study outlines how the technical partners jointly convened public health focal points, including Surveillance, Case Management, Infection Prevention and Control (IPC), RCCE and Points of Entry, from the seven member states in eastern Africa for a practical scenario-based training using a fictitious unknown viral haemorraghic fever outbreak.
The RCCE Collective hope that, by sharing learnings through the technical case study and other workshop outputs, the model could be used to help strengthen national and cross-border RCCE readiness across other global regions facing disease outbreaks.
We've previously shared the report which can be found on the Collective Service website, with further resources to be uploaded in due course.
The UK-PHRST team and partners are currently delivering 10 research projects. In this update, read about a brand-new ethnographic toolkit for outbreak response produced as part of the online and offline COVID-19 rumours project. You can also read about the Rapid Response to Virus Outbreak (RaViG) project's stakeholder consultation workshop in Kenya.
Ongoing research projects
Community feedback triage toolkit available – Online and offline COVID-19 rumours in Sierra Leone and Tanzania
As part of the UK-PHRST’s research study in Sierra Leone and Tanzania to track rumours and concerns about COVID-19, the project team have now developed an ethnographic toolkit, which can be used to facilitate community workshops and focus group discussions. The toolkit can also be adapted for use in any outbreak.
The toolkit forms part of the final outputs from the research project which also included a series of dissemination workshops across Tanzania and Sierra Leone earlier in the year. The workshops brought together key stakeholders in each country to discuss the study’s findings, gather feedback and initiate conversations with policy makers, governments and communities to improve future community-led interventions in outbreak responses.
Download the toolkits on the UK-PHRST's Global Health Network site
Rapid virus genomics for outbreak investigation stakeholder workshop
In July 2024 the Rapid Response to Virus Outbreaks (RaViG) research team convened a stakeholder consultative workshop with the KEMRI-Welcome Trust Research Programme, Kenyan Ministry of Health, representatives from The East African Mobile Laboratory team, representatives of six Kenyan coastal counties and UK-PHRST to discuss the study’s protocol and familiarise them with the project as a whole.
Led by national stakeholders and the RaViG Team, workshop participants examined coastal counties existing mechanisms to rapidly respond to disease outbreaks and whether adding a portable sequencing system would be logistically feasible and add value during future viral outbreaks.
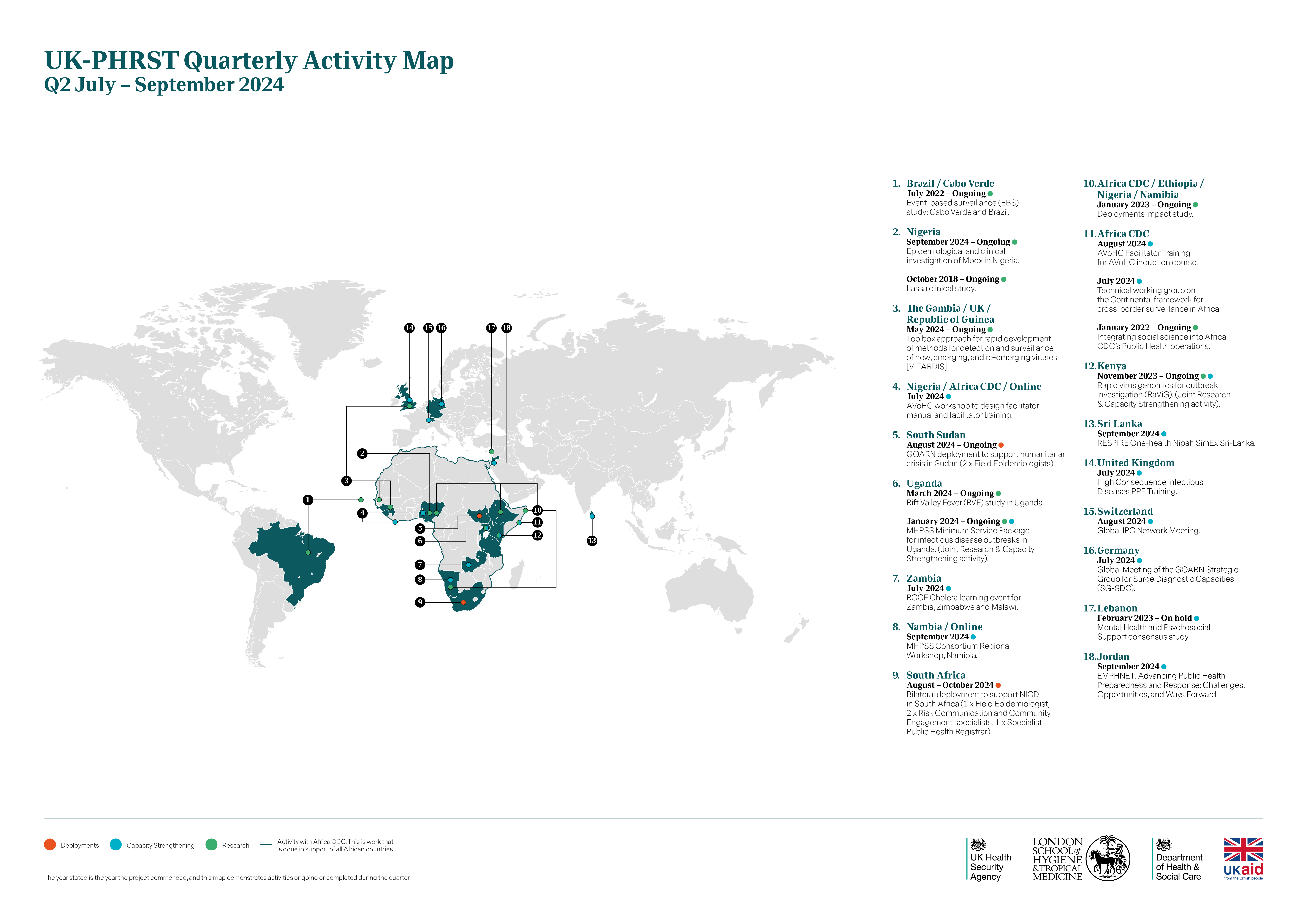
View our quarterly map to see our activities between July and September 2024.
The UK-PHRST has deployed two of its experts to Kinshasa in the Democratic Republic of the Congo (DRC) to support Africa CDC in its response to the ongoing mpox epidemic.
The deployment is supported by the British Embassy in Kinshasa and will involve a UK-PHRST field epidemiologist and an Infection Prevention and Control specialist. Under the direction of the Africa Centres for Disease Control (CDC), the UK-PHRST experts will work in collaboration with other partners to provide a wide range of technical, strategic and tactical inputs to the joint World Health Organization (WHO)-Africa CDC continental incident management team.
Dr Ed Newman, UK-PHRST Director said:
“The UK Public Health Rapid Support team ensures that our expertise in tackling infectious disease outbreaks is rapidly available to support countries who are responding to public health emergencies.
“Our staff will provide specialist support to colleagues at Africa-CDC and the joint continental incident management team as they work to manage the ongoing mpox epidemic, as well as using this learning to further strengthen UK preparedness.”
Africa CDC Director General, H.E Dr. Jean Kaseya said:
"Africa is facing significant public health challenges with the mpox and Marburg virus outbreaks. The UK’s vital support—through both financial assistance and technical expertise—comes at a crucial moment.
This partnership will bolster our efforts to contain these outbreaks, enhance disease surveillance, and strengthen healthcare systems in the Democratic Republic of Congo, Rwanda, and beyond.
Together, we are not just responding to immediate threats, but building stronger, more resilient systems to safeguard the health of millions across the continent."
The deployment comes following the declaration of mpox as a Public Health Emergency of Continental Security by Africa CDC and a Public Health Emergency of International Concern by the World Health Organization (WHO). A recent report from the WHO estimated that there have been over 36,000 suspected cases of mpox in Africa since the beginning of 2024, resulting in almost 1,000 deaths.
This deployment continues the UK-PHRST’s long-standing experience in supporting countries during disease outbreaks at the invitation of a host government or in response to requests made by multinational partners such as Africa CDC, the WHO or via the Global Outbreak Alert and Response Network (GOARN). For example, in recent years, UK-PHRST staff have been deployed to several countries across Africa – including the Democratic Republic of the Congo – to support a range of infectious disease outbreak responses, including Ebola, cholera and yellow fever outbreaks.
The UK-PHRST has also worked closely with Africa CDC over almost a decade to support the creation of its own public health response team – the Africa Volunteer Health Corps.
In addition to the deployment, the UK has announced a financial package of support up to £9million unlocked from the existing Official Development Assistance (ODA) budget, to bolster the national response to mpox in DRC, the epicentre of the mpox outbreak, and across the wider affected region. This includes additional funds to strengthen the UK's existing partnership with UNICEF in DRC. Funds will assist partners to strengthen surveillance systems, reinforce health services and work with communities to raise awareness of risks and personal protective measures, in line with Africa CDC and WHO’s Continental Preparedness and Response Plan.
The UK-PHRST team has been busy delivering capacity strengthening activities, advancing partnerships and contributing to the global discourse around outbreak response. Highlights below:
UK-PHRST successfully delivers its latest Deployment Training

The UK-PHRST’s Capacity Strengthening Team recently delivered the latest edition of its Deployment Training programme to 29 participants from across public health disciplines and institutions, including the UK-PHRST’s Reservist Cadre and six representatives from Africa CDC, from both Head Office and the Regional Coordinating Centres from across the continent.
The training aims to strengthen participants’ knowledge of the UK-PHRST ways of working during deployments, share existing knowledge and experience with peers to deepen awareness and skills, enabling them to work effectively alongside partners and preparing them for deployments by encouraging them to consider the type of challenges and situations they may face.
The training is immersive and structured around a comprehensive scenario that covers different phases of a deployment - from call for assistance, assessment, recommendations and country exit - ensuring a holistic approach to learning.
Read a reflective blog from this year’s organiser.
UK-PHRST assists in multi-country Risk Communication and Community Engagement readiness training in Kenya
To strengthen regional cross-border Risk Communication and Community Engagement (RCCE) readiness during public health emergencies, Africa CDC, UNICEF, International Federation of the Red Cross and the World Health Organization (the Collective Service core partners) as well as International Organization for Migration, READY Initiative and the UK-PHRST, organised a scenario-based training in April 2024 in Mombasa, Kenya.
The UK-PHRST’s RCCE Specialist, Sophie Everest, provided technical support and helped facilitate the sessions which aimed to help strengthen national and cross-border RCCE readiness for outbreak response in Kenya, Somalia, Ethiopia, South Sudan, Uganda, Rwanda and Tanzania.
A summary report and technical case study of the training and associated learnings are available on the Collective Service website.
Somaliland Ministry of Health and Development delegation visit

Following the three-month UK-PHRST bilateral deployment with the Somaliland Ministry of Health Development (MoHD), their Director General and delegates made a visit to London to meet with the UK-PHRST and other UK-based partners.
During the meeting, the Director General, UK-PHRST’s Director Ed Newman and other senior UK Health Security Health Agency officials discussed the public health situation in Somaliland, the recent deployment and explored areas for potential future collaboration.
The UK-PHRST team and partners are currently delivering 10 research projects. In this edition, read about the Community Leader Event Based Surveillance project's launch, training workshops and first mini-guides for health professionals. You can also read about the Marburg project's recent prize at London School of Hygiene & Tropical Medicine Centre for Epidemic Preparedness and Response Awards.
Ongoing research projects
Project launch for Community Leader Event Based Surveillance study in Brazil and The Republic of Cabo Verde, Brasília

The Guardians of Health – Community Leaders research project, officially launched in Brasília and on-line in April 2024, is piloting an early warning system for infectious disease outbreaks in Brazil and Cabo Verde that is developed with and relies on the participation of community leaders.
The study is investigating whether a community-led event-based surveillance system is feasible and more effective at detecting outbreaks of infectious disease than conventional surveillance systems. It also aims to understand how sustainable this approach could be, and whether the involvement of community leaders in the design of the data reporting system from the beginning can help the system to be integrated into local and national public health surveillance in the longer-term.
The launch event included speakers from contributing partners and organisers, including:
- The Brazilian and Cabo Verdean Ministries of Health
- Melanie Hopkins, the British Deputy Head of Mission in Brazil
- José Pedro Máximo Chantre D’Oliveira, the Ambassador of The Republic of Cabo Verde in Brazil
- National Institute of Public Health of Cabo Verde
- Association of Field Epidemiology Professionals (ProEpi)
- Health Situation Room of the University of Brasília (SDS UnB),
- Pan American Health Organization (PAHO)
- Africa CDC
- UK Public Health Rapid Support Team (UK-PHRST)
Read the full story in Portuguese.
Watch the launch event recording.
Community Leader Event Based Surveillance: Study workshops in Cabo Verde

Since the launch event in April, the National Institute of Public Health (INSP) and the Brazilian Association of Field Epidemiology Professionals (ProEpi) held the first training session on the use of the electronic Public Health Emergency Management (ePHEM) software in Cabo Verde in June as part of the Guardians of Health: Community Leaders project.
The workshop was attended by key community health leaders in Cabo Verde who were able to learn about the concept of Event-Based Surveillance and test the ePHEM system in person. Following this workshop, two large user workshops will be held (Santiago South and Santiago North) to test the application throughout the island of Santiago.
Read the full round-up in Portuguese.
Community Leader Event Based Surveillance: Mini-guides for health professionals
The project team have also developed two mini-guides for health professionals and those interested in event-based surveillance with community leaders and approaches to mapping local community leaders as part of public health surveillance projects and/or for programme planning.
Mini guide: Mapping community leaders for local public health surveillance.
Mini guide: Event based surveillance in public health.
London School of Hygiene & Tropical Medicine Centre for Epidemic Preparedness & Response Prizes 2024 - Collaboration Prize winner
We're pleased to share that a UK-PHRST research project recently won LSHTM’s Centre for Epidemic Preparedness and Response 2024 Collaboration Prize.
The project, “A novel One Health approach to develop an early warning system to improve preparedness for and response to Marburg virus disease outbreaks”, involves a multi-disciplinary team of researchers is led by Dr Joseph Akoi Boré at the Centre de Recherche et d'Analyse Médicale (CRAM) in Guinea and involves the UK-PHRST, the University of Oxford, CEFORPAG (Center of Research on Priority Diseases) Guinea, the National Viral Haemorrhagic Fever Reference Laboratory Guinea, the University of Glasgow, Universidad Peruana Cayetano and the MRC Unit The Gambia at LSHTM. The entire team and project was recognised for showcasing the best of contemporary work in the field of epidemic preparedness.
The team has used the award to invest in solar panels for Dr Joseph Akoi Boré’s laboratory, further enhancing sustainability and team capacity to continue researching viral outbreaks in Guinea.
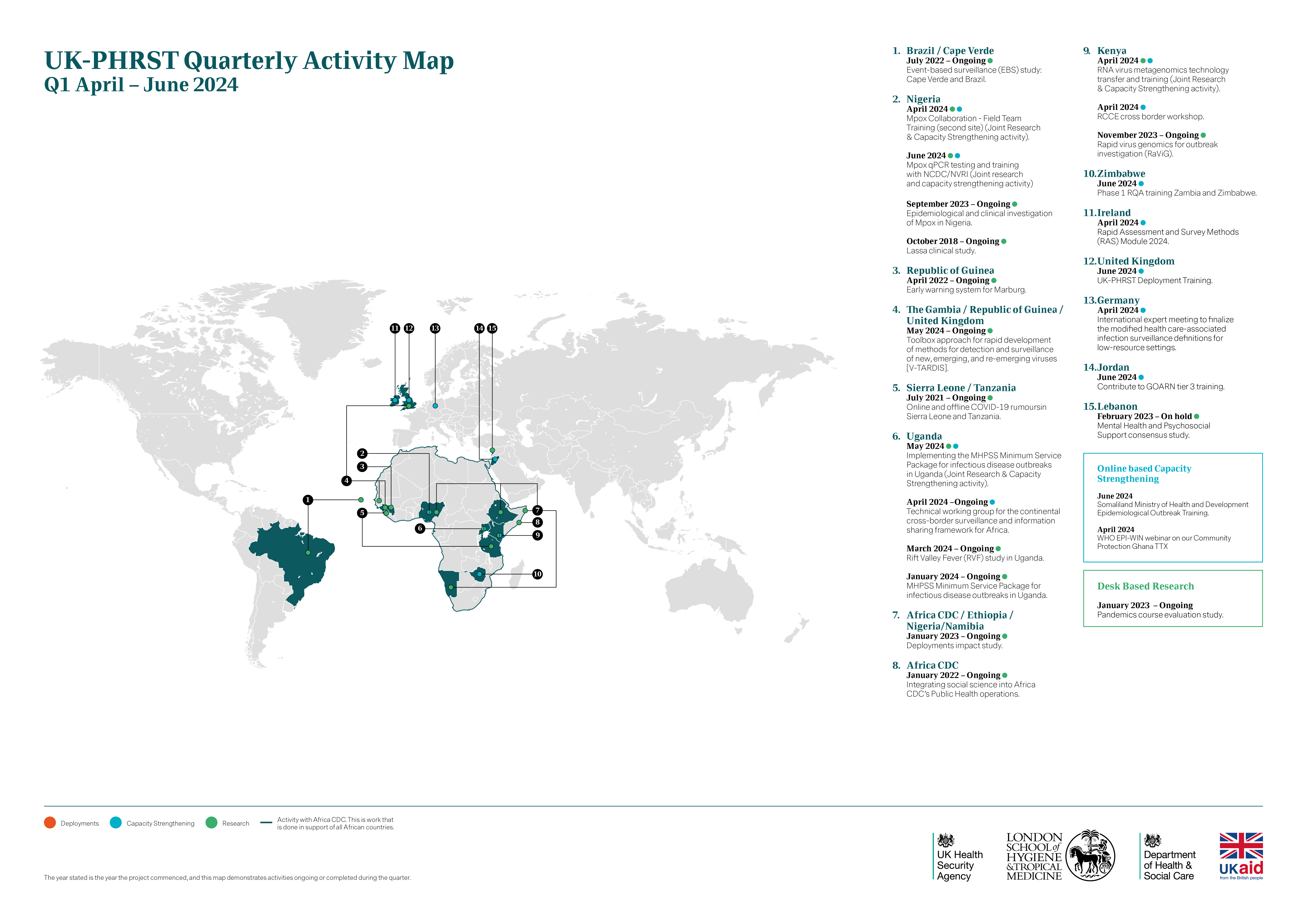
View our quarterly map to see our activities between April and June 2024.
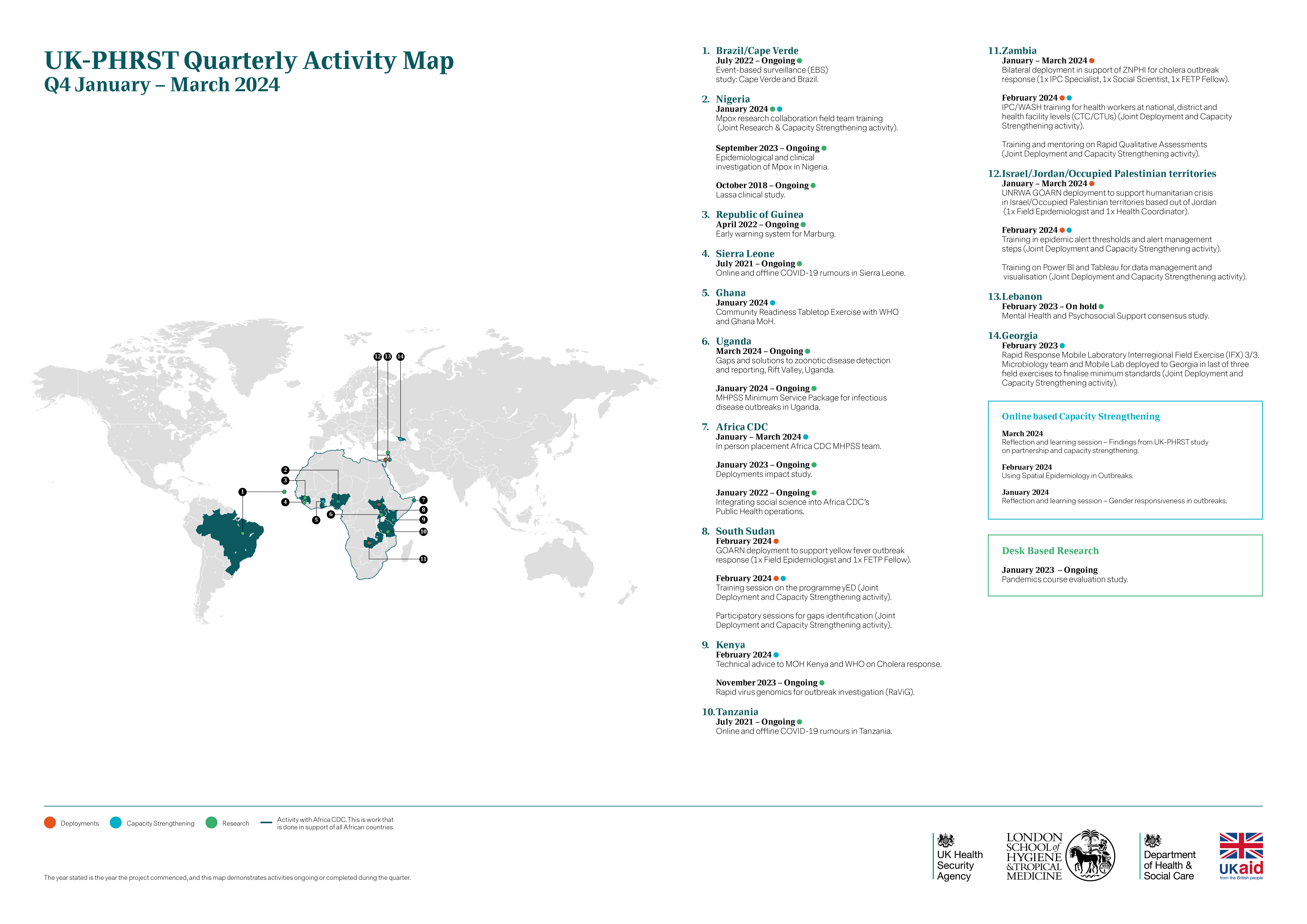
View our quarterly map to see our activities between January and March 2024.
Rapid virus genomics for outbreak investigation (RaViG) - proof of principle in Coastal Kenya

In February, members of the UK-PHRST’s research team joined collaborators at the KEMRI-Wellcome Trust Research Project in Kenya to launch a new research project: Rapid virus genomics for outbreak investigation (RaViG) - proof of principle in Coastal Kenya.
The project, a collaboration between the KEMRI-Wellcome Trust Research Programme in Kilifi, Kenya (KWTRP), the UK-PHRST, the Kenya Ministry of Health and six coastal counties, will assess whether deploying portable whole genome sequencing in real-time during outbreaks is feasible, and if this provides added value to conventional outbreak response approaches.
Coastal Kenya has experienced recurrent outbreaks of various diseases including dengue, measles, norovirus, influenza, and COVID-19. However, there is limited knowledge regarding the origin, transmission patterns, and dispersal dynamics of these outbreaks. Furthermore, there is limited existing for real-time analysis.
To build the evidence base, the project team will co-ordinate with county public health teams in coastal Kenya to trial deploying a portable whole genome sequencing system alongside their conventional outbreak responses to diseases of suspected or confirmed viral origin.
The UK-PHRST will support and advise on setting up portable whole genome sequencing in the field during outbreak response and support scientific evaluation and interpretation throughout the study.
Professor Gwenda Hughes, UK-PHRST Director of Research said: “We are delighted to be part of this exciting research collaboration with the KEMRI-Wellcome Trust Research Programme, Kenya Ministry of Health and county public health teams to assess if using a portable sequencing system to uncover the genome of pathogens in real-time can strengthen outbreak response in Kenya.”
Sharing the findings of our research on COVID-19 rumours to improve community trust and engagement in future disease outbreaks

Between 2021 and 2024, the UK-PHRST undertook a study in Sierra Leone and Tanzania to track rumours and concerns about COVID-19, with the aim to better understand the relative influence and mechanisms of online and offline rumours regarding COVID-19 and to identify solutions to address community concerns during health emergencies. The study used qualitative social science research techniques including community ethnography, interactive workshops, and key informant interviews to gain a deep insight into circulating rumours, how they are shared in social networks and to explore communities’ perspectives of and trust in different sources of information.
Marking the conclusion of the project, three dissemination workshops took place in Tanzania and Sierra Leone in March 2024. The workshops brought together key stakeholders in each country to discuss the study’s findings, gather feedback and initiate conversations with policy makers, governments and communities to improve future community-led interventions in outbreak responses.
In Dodoma, Tanzania, the workshop was opened by Ministry of Health (MoH) and National Institute of Medical Research (NIMR) senior staff. Project results and draft conclusions were presented and there was broader discussion of social science, community engagement and infodemic management in Tanzania after the study-specific presentations and discussions.
Two workshops were held in Sierra Leone, the first of which was held at held in Freetown targeting national level stakeholders from the MoH, the National Public Health Agency (NPHA), WHO and international and local NGO’s and CSOs actively involved in Risk Communications and in Community Engagement (RCCE) interventions in Sierra Loene. The second workshop in Kambia brought together district level stakeholders including officials from the District Health Management Team (DHMT), local authorities, traditional healers, study participants, religious leaders, university students and ordinary citizens. In both workshops, findings from the study were shared with participants followed by plenary sessions to discuss findings and kick start conversations about how the findings can be utilised to inform local RCCE programmes and future research. In addition, the workshops established next steps to address these challenges using innovative methods based on the research project’s data.
Fostering community readiness to respond to public health emergencies in Ghana
In Ghana, a three-day community readiness simulation exercise, co-organized by the Ministry of Health, Ghana, the World Health Organization, and the UK-PHRST brought together stakeholders from health, local government, disaster management, animal and environment sectors, drawn from the Eastern region of Ghana to test communities’ preparedness and emergency procedures and response plans.
The community readiness simulation exercise was aimed at enabling stakeholders to identify strengths, gaps and reflect on priorities that will help strengthens communities’ readiness, working with the health workforce to detect, notify and respond to public health threats before they escalate.
Dr Claire Bayntun, UK-PHRST Head of Capacity Strengthening said: “We are delighted to be part of this exciting collaboration between the World Health Organization, the Ministry of Health in Ghana and other partners. We have contributed our technical expertise to this tabletop simulation exercise which will ultimately help local communities be better prepared for outbreaks in the future.
The outcome of this exercise will not only benefit Ghana - the learnings will also be relevant for the public health responses for communities in many other countries.”
Read the news story from WHO Ghana here.
RRML IFX Round-up

The UK-PHRST microbiology team recently took part in the first ever Interregional Field Simulation Exercise (IFX): a three-part exercise to review and test the proposed minimum standards across the whole RRML life cycle, from pre-deployment, during outbreak response and end-of-mission phases. The team worked alongside other international teams to test-run co-deploying mobile lab equipment and expertise through exercises in Germany, Türkiye and Georgia. The exercise also tested how RRMLs work alongside other WHO health emergency workforce assets, such as Emergency Medical Teams (EMTs), just as in a real outbreak.
- Read more

View our quarterly map to see our activities between October and December 2023.
- Read more
UK-PHRST team and partners are currently delivering ten research projects, a selection of which are highlighted below.
UK-PHRST Panel Discussion and Q&A: Working with family caregivers to improve infection prevention and control in hospitals
This discussion and Q&A event, aimed at those working in health service delivery, policy development, health workers, Infection Prevention and Control teams and other academics, examined the role of caregivers in African healthcare systems, an often integral but largely unrecognised part of the health team.
The event began with presentations focusing on the healthcare situation in Cameroon and Malawi specifically delivered by researchers from a variety of organisations including the UK-Public Health Rapid Support Team, the Cameroon Baptist Convention Health Service/Infection Control Africa Network, WaterAid and London School of Hygiene & Tropical Medicine.
There followed a chaired panel Q&A session with leading experts in the field, chaired by Professor Wendy Graham, an LSHTM Professor of Obstetric Epidemiology. The event was an opportunity to find out about the next steps for the research and its real-world implementation.
Event Based Surveillance Study - Cape Verde and Brazil workshops

Brazil workshop participants. Image credit: ProEpi/Mariana Ferreira Lopes 
Cape Verde workshop participants. Image credit: INSP (Instituto Nacional de Saúde Pública de Cabo Verde)/Dárcio Vasconcelos. Throughout November and December 2023, the project team held workshops in both Cape Verde and Brazil. In Cape Verde, the team met with ten community leaders who helped test the project app Guardians of Health that will be used to record the event-based disease surveillance information collected directly from communities.
The team held two workshops in Brasilia working with local community leaders to introduce the study and map out potential local individuals who could participate in data collection. Both workshops were an opportunity to engage local leaders in the project, creating a bond with the local community to enable their full participation and ensure they lead the nomination of participants using their understanding of regional dynamics. The team now intend to invite the nominated leaders to a future project development workshop as well as visiting the local territories and building stronger community bonds within the study regions.
- Read more
UK-PHRST attends CPHIA Conference 2023: Repositioning Africa in the global health architecture

CPHIA 2023 conference banner. Credit: Lucy Trelfa In November, UK-PHRST members attended the 3rd 2023 International Conference on Public Health in Africa (CPHIA) in Lusaka, Zambia alongside thousands of delegates from across Africa and further afield. They launched a Global Health Diplomacy course which was developed with Africa CDC, discussed how best to respond to infectious disease outbreaks and strengthened our partnership with Africa CDC to support mental health across the continent. This annual conference provides a unique African-led platform for public health leaders across the continent to reflect on lessons learned in health and science and align on a way forward for creating more resilient health systems.
Dr Ed Newman, UK-PHRST Director said:
“This year’s International Conference on Public Health in Africa was a great opportunity for the UK-PHRST to support our Africa-CDC colleagues with their events and partake in some critical side events ourselves – further building on the excellent relationships we have in the region. I was especially pleased to see the emphasis on African health leadership to build solutions for the continent’s public health challenges, particularly exemplified by the close alliance demonstrated by Africa CDC and WHO Senior leadership. We support their clear call for nationally driven, local responses to public health threats - further emphasising the value that both organisations place on collaboration."
See the pictures from the event.
Interregional One Health cross-border simulation exercise

Credit: World Health Organization Ethiopia At the request of the World Health Organization (WHO) Ethiopia country office, UKHSA teams including the UK-PHRST, mobilised to help deliver a unique and complex One Health cross-border simulation exercise between Ethiopia, Somalia and Kenya, that was held in Addis Ababa in October 2023.
UK-PHRST colleagues alongside others from the UKHSA’s International Health Regulations Strengthening Project (IHR-SP) based in both the UK and Ethiopia, and UKHSA’s Global Health Consultants joined forces with stakeholders from across the three countries and other international partners to test preparedness, operational readiness, and cross-border and cross-sector coordination in the event of a One Health-related threat – in this case, anthrax.Hibo Asad a Field Epidemiologist with the UK-PHRST, reflected on her experience:
“A key highlight for me was the inclusion of the community representatives across Ethiopia, Kenya and Somalia – facilitated by Risk Communication and Community Engagement (RCCE) Colleagues in the UK-PHRST. This is the first time we have held a workshop of this magnitude with community representatives involved and contributing to discussions on cross-border preparedness and coordination against One Health threats. Their shared perspectives significantly strengthened the One Health discussions, bringing to the table very insightful on the ground experience and wisdom.”
The simulation exercise was well received by all participants, with community experts applauding “the sharing of expertise and resources to collaborate in achieving a common goal”.
Dr Lilian Wambua, Regional One Health Coordinator at the World Organization for Animal Health, also praised the cross-organisational work in her closing remarks, saying:
“Thanks to colleagues from WHO, UKHSA, PANDORA and other organisers. The level of inclusivity has been phenomenal, from community to high-level policy makers, all allowing for smooth partnership working.”
The findings from the exercise are currently being evaluated and written up. These will be shared with key country stakeholders to start taking the next steps towards cross-border health security using a One Health approach.
- Read more
The UK-PHRST team has been busy delivering capacity strengthening activities advancing partnerships and contributing to the global discourse around outbreak response. A selection are highlighted below:
UK-PHRST supports Africa CDC’s Regional Francophone workshop on Mental Health and Psychosocial Support (MHPSS) Emergency Preparedness and Response
Credit: Africa CDC 
Credit: Africa CDC In September 2023, Africa CDC arranged a third regional workshop in Togo as it continues to build recognition for the importance of MHPSS in outbreaks across the African continent, focusing this time on Francophone countries in Central and West Africa. The event was part of a series of workshops, previously held in Liberia and Kenya, and was attended by 49 individuals spanning 20 countries including national leads in mental health and Emergency Preparedness and Response alongside input from the Inter-Agency Standing Committee, the UK-PHRST, UNICEF, and other regional bodies.
Julian Eaton, Co-Lead, UK-PHRST Mental Health Psychosocial Support Group attended the workshop on behalf of the UK-PHRST and said:
“National health and other sector leaders deserve coordinated and evidence-based information to drive effective response. Our international partnership with Africa CDC, WHO and regional public health institutes has proven an incredibly valuable way to support national emergency preparedness in mental health and psychosocial support.”
The workshop provided a unique opportunity to invest in learning and sharing specific evidence in French. Although around 300 million people in Africa live in Francophone countries, there is a relative lack of investment in mental health and psychosocial support in this community, something this workshop aimed to start addressing.
The series are based around a Theory of Change model, with learnings incorporated iteratively through each workshop as well as using evidence systematically gathered from other sources – ultimately aiming to support national mental health and Emergency Preparedness and Response (EPR) teams to better plan and build stronger systems for response in the event of future emergencies.Build Better Before: Scaling up capacities for Mental Health and Psychosocial Support Preparedness and Risk Reduction

Credit: World Health Organization Europe. 
Credit: World Health Organization Europe. Biksegn Yirdaw, Assistant Professor in Mental Health and a member of our Mental Health and Psychosocial Support (MHPSS) team, attended a World Health Organisation international workshop held in collaboration with the Estonian government: “Build Better Before: Scaling up capacities for Mental Health and Psychosocial Support (MHPSS) Preparedness and Risk Reduction” on behalf of the UK-PHRST in September. The workshop lasted several days and included lecture session and a full-scale simulation exercise on MHPSS preparedness and response, disaster risk management (DRM) and emergency preparedness and response (EPR) in humanitarian/emergency situations.
Biksegn was involved in facilitating MHPSS need assessments, writing a standard operating procedure and developing a response plan during the simulation exercise. As a result, he deepened his expertise in conducting rapid need assessments, risk analysis, and planning during emergency situations. Using this knowledge, he will help the UK-PHRST further strengthen its MHPSS component of its outbreak response work in Overseas Development Assistance eligible countries around the world.
Bringing together more than 80 MHPSS and humanitarian experts from 35 countries, the workshop aimed to strengthen the capacities of responding organisations to integrate MHPSS into national emergency plans and to include MHPSS as part of real-world emergency response including to infectious disease outbreaks. In particular, the workshop’s approach could be used to inform the UK-PHRST’s work to design, implement and evaluate integrated MHPSS interventions in infectious disease outbreaks – ultimately progressing the team’s research portfolio and ensuring the UK-PHRST’s work can have a global impact.
Find out more about the UK-PHRST's MHPSS work.
International Conference on Infection Prevention and Control (IPC), Geneva
IPC colleagues Emilio Hornsey and Lipi Begum recently presented their poster on the review of IPC activities during outbreak response deployments by UKPHRST in 2022 at the biennial, International Conference on Infection Prevention and Control in Geneva, Switzerland. The event not only allowed international networking with academic and operational IPC colleagues but also highlighted how other governments, NGOs & civil societies manage health sector resilience and patient safety via IPC during normal and emergency outbreak responses.
- Read more
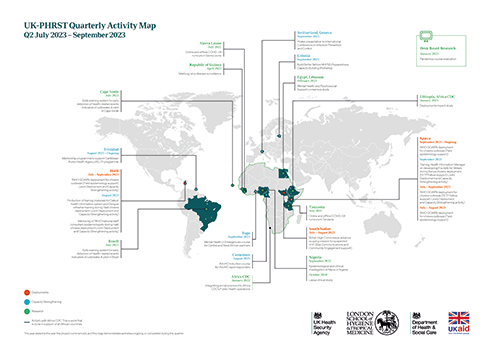
View our quarterly map to see our activities between July and September 2023.
- Read more
The UK-PHRST team and partners are currently delivering 10 research projects, a selection of which are included below:
Nigeria mpox research collaboration launches

Credit: Nigeria CDC Researchers from the Nigeria Centre for Disease Control (NCDC) and the UK-Public Health Rapid Support Team (UK-PHRST) are teaming up with multiple partners for a new project to study mpox in Nigeria. Since it re-emerged in Nigeria in 2017, the mpox virus has caused numerous outbreaks globally. This research aims to increase understanding of how it spreads and affects communities in Nigeria.
NCDC, alongside partners including the UK-PHRST, the National Veterinary Research Institute (NVRI), the Niger Delta University Teaching Hospital (NDUTH), the Pandemic Sciences Institute at the University of Oxford and stakeholders in Lagos and Rivers States, launched the collaborative project at an event in Abuja on 16 October. Distinguished guests included senior national and state representatives from collaborating stakeholders and partners across Nigeria and from the UK.
The co-created research project – titled “Epidemiological and clinical investigation of mpox in Nigeria: A multi-disciplinary research project to inform case management and outbreak prevention and control” - will help address the current significant gaps in clinical and epidemiological knowledge of the virus in Nigeria. Its findings have the potential to not only strengthen detection, prevention, response, and control in Nigeria, but also inform practice in other countries across the world where mpox is endemic.
Following the launch of the research project, the UK-PHRST will continue to support Nigerian partners in the co-ordination and implementation of the study, lab capacity strengthening and data analysis.Professor Gwenda Hughes, co-project lead, Deputy Director for Research for UK-PHRST, and Professor of Epidemiology and Public Health at LSHTM said:
“The UK Public Health Rapid Support Team is delighted to be part of this exciting collaboration between Nigeria Centre for Disease Control and other partners to better understand the clinical characteristics, pattern of infection and spread of mpox in Nigeria – a disease that has greatly affected Nigerian communities, especially in recent years.
“The UK-PHRST will support Nigerian colleagues to answer important scientific questions through this extensive research programme and will also help deliver training of local laboratory staff and field teams. Our microbiology specialists have already provided lab equipment and shared expertise to help build local diagnostic capabilities for mpox. Ultimately, through co-creation and by taking a partner-led approach with our Nigerian colleagues, our aim is to support improved case and contact management and inform the development of effective control measures for mpox both in Nigeria and globally.”Read the full NCDC press release.
Online and offline COVID-19 rumours in Sierra Leone and Tanzania
In August 2023, the research team completed both data collection and analysis in Sierra Leone and Tanzania. The project team are currently developing an ethnographic toolkit and writing up results. Project dissemination will take place in the New Year.
Rapid Virus Genomics for Outbreak Investigation (RAViG) – Assessing the feasibility and added value in Coastal Kenya
A new study, in partnership with the KEMRI-Wellcome Trust Research Programme, Kilifi, Kenya began in October. The central aim of the project is to assess the implementation of real-time field genomics (“portable sequencing”) to support investigation and management of suspected viral outbreaks in coastal Kenya. The investigating team aim to add to the evidence base on the added value and sustainability of in-field rapid genomic sequencing relative to conventional surveillance in low resource settings. The team will explore how genomic data can help identify the cause of an outbreak or factors associated with it, and whether this information can influence policy or outbreak control measures. The project team will also work with the Kenyan Ministry of Health, Africa CDC, and the Regional WHO in delivering this research.
- Read more

Image credit: NCDC Comms Researchers from the Nigeria Centre for Disease Control (NCDC) and the UK-Public Health Rapid Support Team (UK-PHRST) are teaming up with multiple partners for a new project to study mpox in Nigeria. The virus has caused a number of outbreaks since it re-emerged in Nigeria in 2017, and this research aims to increase understanding of how it spreads and affects people among Nigerian communities.
Nigeria Centre for Disease Control (NCDC), alongside partners including the UK-PHRST, the National Veterinary Research Institute (NVRI), the Niger Delta University Teaching Hospital (NDUTH), the Pandemic Sciences Institute at the University of Oxford and stakeholders in Lagos and Rivers States, launched the collaborative project at an event in Abuja on 16 October. Distinguished guests included senior national and state representatives from collaborating stakeholders and partners across Nigeria and from the UK.

Image credit: NCDC Comms The co-created research project – titled “Epidemiological and clinical investigation of mpox in Nigeria: A multi-disciplinary research project to inform case management and outbreak prevention and control” - will help address the current significant gaps in clinical and epidemiological knowledge that surround the virus. Its findings have the potential to not only strengthen detection, prevention, response, and control in Nigeria, but also inform practice in other countries across the world where mpox is endemic.
The research will be split into two linked studies: a clinical study and a One Health study. These will be implemented concurrently to understand the clinical characteristics, patterns and routes of infection and associated risk factors, and the experiences of people with confirmed mpox and those close to them.
Dr Ifedayo Adetifa, Director General of the NCDC, said: "Today, we begin the journey of knowledge, unity, and determination. In partnership with dedicated researchers and institutions, we set out to unravel the unknowns of the mpox virus through bridging clinical and One Health studies. This project symbolises our unwavering commitment to protecting the health of Nigerians, and in turn the world, embracing the power of research, and the strength of collaboration. As we work together, may we move closer to a world free from the threat of mpox that ensures the wellbeing of generations to come."
Using £1.6 million funding provided by the UK Department of Health and Social Care through UK Aid, the UK-PHRST – an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine (LSHTM) - has worked closely with the partners to co-create the research project. The collaborating organisations first met in early 2022, prior to the global mpox outbreak, to agree to co-develop a preparedness-and-response research programme on mpox in Nigeria. Following the launch of the research project, the UK-PHRST will continue to support Nigerian partners in various parts of the study from design, co-ordination and implementation, lab capacity strengthening to data analysis and publication. This will ultimately enable Nigerian partners to provide the necessary long-term laboratory support and promote sustainable mpox diagnostics in Nigeria.
Professor Gwenda Hughes, co-project lead, Deputy Director for Research for UK-PHRST, and Professor of Epidemiology and Public Health at LSHTM, said: “The UK Public Health Rapid Support Team is delighted to be part of this exciting collaboration between Nigeria Centre for Disease Control and other partners to better understand the clinical characteristics, pattern of infection and spread of mpox in Nigeria – a disease that has greatly affected Nigerian communities, especially in recent years.
“The UK-PHRST will support Nigerian colleagues to answer important scientific questions through this extensive research programme and will also help deliver training of local laboratory staff and field teams. Our microbiology specialists have already provided lab equipment and shared expertise to help build local diagnostic capabilities for mpox. Ultimately, through co-creation and by taking a partner-led approach with our Nigerian colleagues, our aim is to support improved case and contact management and inform the development of effective control measures for mpox both in Nigeria and globally.”
Image credit: NCDC Comms In his address at the launch event, Dr Edmund Newman, Director of the UK-PHRST, said: “It is great to see this project and collaboration between UK-PHRST and our Nigerian partners progressing to a point where we can launch our co-created mpox study. This has been possible thanks to significant work from all sides and builds upon the long history of the UK-PHRST’s successful work with Nigerian partners including Nigeria CDC which has evolved from bilateral support missions and more recent capacity strengthening work. We will continue to support our Nigerian colleagues as they lead the way on this flagship project to answer the important research questions about mpox in Nigeria.”
Mpox virus, formerly known as monkeypox, causes the most important global human orthopoxvirus disease since smallpox was eradicated in 1979. Since the virus re-emerged in Nigeria in 2017, reported cases have continued to increase annually. From 2017 until now, there have been 2668 suspected cases, 975 confirmed cases and 14 deaths, with Lagos and Rivers States accounting for the highest burden of the disease. As such, the research project will be implemented in Lagos and Rivers states in the first instance.
The 2022 global outbreak which affected over 100 countries coincided with Nigeria’s largest outbreak with 762 confirmed from more than 2000 suspected cases. While this sharp rise in cases is likely linked to improved surveillance and testing, for Nigeria and other endemic countries, the surge of mpox attention and information only further highlighted important gaps in clinical and epidemiological knowledge and the effect of this deficit on developing effective measures to prevent further cases. The research project aims to answer the co-identified research questions for Nigeria, while also informing practice in similar endemic settings.
Read the full NCDC press release about the event.
About NCDC
The Nigeria Centre for Disease Control and Prevention (NCDC) is the country’s national public health institute, with the mandate to lead the preparedness, detection, and response to public health emergencies. The Bill for an Act to establish NCDC was signed into law in November 2018 by President Muhammadu Buhari. The mission of the NCDC is to protect the health of Nigerians through evidence-based prevention, integrated disease surveillance and response, using a One Health approach, guided by research, and led by a skilled workforce.
Launch event attendeesThe project launch event took place on 16 October 2023 in Abuja and included the following key guests amongst many others:
- Representatives of:
- Director General of Nigeria CDC
- British High Commissioner to Nigeria
- Federal Ministry of Agriculture and Food Security
- Federal Ministry of Environment
- Chief Veterinary Officer of Nigeria
- University of Port Harcourt Teaching Hospital
- Ministry of Defence Health Implementation Programme
- UK Health Security Agency (UKHSA) and UKHSA IHR Strengthening Programme
- Wild Aid
- Walter Reed Program - Nigeria/Henry Jackson Foundation Medical Research Institute
- Director of Public Health, Rivers State Ministry of Health
- The Honourable Coordinating Minister for Health and Social Welfare
- The Honourable Commissioner of Rivers State Ministry of Health
- The Chief Medical Directors of Rivers State University Teaching Hospital and Lagos University Teaching Hospital
- The President and the Acting Registrar of Veterinary Council of Nigeria
- The Director/Chief Executive of National Veterinary Research Institute,
- The Directors of Veterinary Services of Lagos State Ministry of Agriculture and Rivers State Ministry of Agriculture
- The Conservator General of National Park Service Abuja
- The Director, Public Health Laboratory Services
- The Director of Public Health, Rivers State Ministry of Health
- The State Epidemiologist, Rivers State Ministry of Health
- Disease Surveillance and Notification Officers and Clinical Health Workers from Lagos and Rivers States
- UK-PHRST speakers included:
- Co-principal Investigator
- UK-PHRST Director
- Representatives of:
- Read more
Julian Eaton. Co-Lead, UK-PHRST Mental Health Psychosocial Support Group
In the face of a public health emergency such as a major disease outbreak, governments and responding organisations know they must implement public health measures to quickly control the situation and prevent loss of life. As we know all too well from COVID-19, cholera, Ebola and other disease outbreaks, infections which spread rapidly can have devastating physical impacts. There is, however, a less visible effect of these outbreaks on people’s mental health, something which is beginning to be addressed by specialists in Mental Health and Psychosocial Support (MHPSS) like the UK-Public Health Rapid Support Team’s dedicated MHPSS team.
Even outside of an emergency situation, mental health is often not part of public health measures and services are often not on par with the standard of care given to those with physical injuries. Emergencies of all kinds can increase the risk of physical and mental health problems, especially if people are displaced, so it is imperative that mental health is addressed in these circumstances.
World Mental Health Day is an opportunity to remember the importance of mental health as an essential component of global public health in both everyday and emergency situations. Although huge strides have been made to make sure mental health is not left out of outbreak response, there's still more to do before it's integrated into every health emergency response; from outbreak preparedness activities, climate change and other natural hazards and conflicts.
This year’s theme of ‘Mental health is a universal human right’, reaffirms the importance of understanding how central mental health is to achieving Universal Health Coverage - to ensure that everyone, especially the most vulnerable, has access to the care they need, even during a public health emergency.
The road to establishing best practice in MHPSS
Almost 20 years ago, the Inter-Agency Standing Committee Guidelines on MHPSS in Emergency Settings, laid the foundations for best practice in MHPSS, stimulated by the need to apply global best practice standards in times when people are most vulnerable. The principles it laid down have served the field well, and the MHPSS community has an increasing range of evidence-based tools, including the Minimum Service Package (hosted at the Mental Health Innovation Network at London School of Hygiene and Tropical Medicine). A new research agenda for 2021-2030 was recently outlined, which demonstrated how far we have come, particularly in understanding the extent of needs and the basic elements of what works to reduce suffering. A mechanism is in place to quickly provide effective coordination in emergencies under Inter-agency Standing Committee (IASC), a surge support capacity is run by the Dutch government on behalf of the MHPSS community, and other key public health agencies like Africa CDC are also putting this in place alongside their response to physical health needs.
Learning lessons from COVID-19 and beyond
The COVID-19 pandemic demonstrated both increased mental health needs, and the importance of a range of health responses; from the value of neighbours looking out for each other’s basic needs, to health organisations having to protect access to essential mental health care services that were at risk. Despite the development of good quality guidance during COVID-19, when the MHPSS community was very nimble in its response, there remain substantial gaps in evidence of what works, and in sufficient political buy-in to invest in and act on risks to mental wellbeing in emergencies. People with pre-existing mental health conditions are far more negatively impacted by outbreaks than others, and there is always a huge increase in distress and mental health needs during outbreaks among the general population, and importantly, health and other sector response organisations. There are a number of reasons behind this: anxiety about contracting infection or getting vaccinated; some direct physical, emotional and cognitive effects (for example as part of long COVID); stigma and social exclusion associated with infection; and probably most significantly, the impact of social changes like isolation, economic loss, or educational disruption, especially when these are over prolonged periods.
How the UK-PHRST is making MHPSS part of outbreak response
The UK-PHRST strives in all areas of its work to create lasting change in response to infectious disease outbreaks across the globe by putting emphasis on knowledge co-creation, global partnerships and real-world action. This is no different for the UK-PHRST’s MHPSS team. Through our innovative research, capacity strengthening efforts and advocacy for on-the-ground response work, the MHPSS team works to bring mental health interventions to the fore of outbreak response and empower countries across Africa, Official Development Assistance (ODA) eligible countries and the wider global community to create real and lasting positive change for those affected by mental health problems following an infectious disease outbreak.
The UK-Public Health Rapid Support team has a dedicated MHPSS group, focused on research, capacity building, and deployment in the intersection of mental health, wellbeing and infectious disease outbreaks. Our work includes:
- Strengthening MHPSS preparedness and response at national level through collaborating with public health institutions like Africa CDC, WHO, Inter Agency Standing Committee, West African Health Organization, East Central and Southern Africa Health Community and other agencies
- Research, with a specific focus on understanding what works in MHPSS preparedness and response at country level, through participatory implementation research. Our aim is to equip decision-makers with clear, evidence-based guidance for integration MHPSS into outbreak response. To date we have published assessments of strength of outbreak preparedness across Africa, reviews of literature, and are planning implementation research in Africa.
- Strengthening deployment mechanisms for rapid response, through collaboration with the African Volunteer Health Corps and IASC/Dutch Surge Support mechanisms
- Building networks of MHPSS and Emergency Preparedness and Response partners for ongoing peer support, learning and coordination
- Supporting responder wellbeing within the RST and across other outbreak response partners
All of these workstreams contribute to one overall aim; to understand better the factors that influence how people respond to crisis, and to equip government and non-governmental organisations to be prepared and able to respond effectively to the mental health needs of people that come about from future public health emergencies like infectious disease outbreaks.
With so much progress in recent years around the world on mental health, the UK-PHRST MHPSS team is working hard to keep up the momentum and integrate mental health measures into outbreak response so that no one is forgotten, especially during an emergency.
Work with the UK-PHRST MHPSS team
Find out more about the MHPSS team within the UK-PHRST.
If you or your organization would like to collaborate or request MHPSS help during an outbreak, please contact [email protected].
- Read more
UK-PHRST and Partners' Learning Review Video. Credit: lightlounge.co.za The UK-PHRST and its international partners came together to review their previous work, evaluating its strengths and weaknesses as part of a three-day Learning Review Session in Cape Town, South Africa. The discussions, in September 2022, acknowledged the ongoing success and enthusiasm for the UK-PHRST’s partnership working approach and also pointed to key issues that potentially affect the work of the UK-PHRST and international partners. These included strengthening public health leadership, narrowing the North-South technological gap, ensuring deployments create impact for host countries and embedding greater levels of equity across all working relationships.

Image credit: lightlounge.co.za The newly published UK-PHRST and Partners Learning Review Post Review Reflections & Actions Report highlights case studies from the discussions, and provides 35 recommendations for improved ways of working. The UK-PHRST senior leadership responded to 20 of the recommendations which the attendees felt were priority areas.
Learning and improvement are fundamental to the UK-PHRST’s international activities. The Learning Review and associated report will help the UK-PHRST to better understand our partners, their opportunities and challenges, and empower us to collectively address partner identified problems - a sentiment emphasised by UK-PHRST’s Director Ed Newman.
He said: “By giving a voice to our staff and partners to capture and share some of the lessons we identified, and by being candid about the difficulties we encountered - as well as highlighting our many successes - we can continue to work well with our partners, but also learn from those lessons and grow stronger in our collaboration and in the activities we jointly undertake.”

Image credit: lightlounge.co.za Not only was the Learning Review an opportunity for the UK-PHRST and partners to reflect on their previous work and achievements, but it also provided a vital space for mutual and multi-directional learning and capacity strengthening outside of an emergency infectious disease outbreak situation.

Image credit: lightlounge.co.za Dr Maryirene Ibeto and Dr Femi Nzegwu from the UK-PHRST emphasised that: “The review highlights how by having these continuous conversations, low- and middle- income countries and support agencies like the UK-PHRST can share best practice and learn from each other constantly. This will mean that they can more effectively deal with a crisis when it hits – ultimately creating a safer and more secure global health situation for everyone.”

Read the full UK-PHRST and Partners Learning Review Post Review Reflections & Actions Report






- Read more
View our quarterly map to see our activities between January and March 2023.
- Read more
Field Deployment Training course

Credit: UK-PHRST Team This year’s Field Deployment Training (FDT) course took 18 participants on the 'journey' of pre-deployment, deployment, needs assessment, intervention recommendations and exit planning thanks to the expertise of the co-ordinators in humanitarian scenarios, health, operations and capacity strengthening.
The training, jointly delivered by UK-MED (a humanitarian health organization), UK-PHRST and UK Health Security Agency across four days in Bedfordshire, is a mandatory component for all deployable members of the UK-PHRST team to ensure they can deploy safely and effectively.
To make sure the participants would be equipped for situations, the components typical of real deployments were condensed into a micro time scale (ie. experienced across four days rather than the usual deployment of six weeks), using forum theatre techniques such as being accosted by media, being challenged for breaches in security protocol and safe-guarding issues.
Workshop on mpox antibodies detection
There was an opportunity to learn more about tools for detecting mpox at a workshop during the UK-PHRST research team’s visit to Abuja, Nigeria in March focusing on the clinical characteristics and outcomes of mpox disease in Nigeria. The MVA (modified vaccinia Ankara) ELISA assay workshop and technology transfer session was held with colleagues from the Nigeria Centre for Disease Control (NCDC) and National Veterinary Research Institute (NVRI).
The workshop, hosted by The MRC Unit The Gambia at LSHTM, included training and advice from a University of Oxford expert on how to use the MVA ELISA to detect mpox antibodies for different aspects of the study. Colleagues from NCDC – Abuja, NCDC – Lagos, NVRI – Vom, the MRC Unit The Gambia at LSHTM and the National Public Health Laboratory Gambia who attended found the workshop informative, enjoyable and worthwhile.
Caribbean collaboration visit
In March, our Director Ed Newman, was invited to meet counterparts from the Caribbean Public Health Agency (CARPHA). Together, the two organisations hope to develop a strong collaborative relationship which could include the co-deployment of staff at CARPHA’s request - UK-PHRST deploying staff to CARPHA to enhance their public health emergency response and CARPHA deploying staff outside the Caribbean to gain response experience.
The meetings were well received by the CARPHA Senior Leadership who were very keen to work further with the UK-PHRST and develop future areas of collaboration. Additionally, Anita Shah, a UK-PHRST Field Epidemiologist who had seconded to CARPHA, shared the findings of her work with the organisation regarding its Field Epidemiology and Laboratory Training programme and future expansion plans.
- Read more
Ongoing research projects
The UK-PHRST are currently delivering eight ongoing research projects, a selection of which are included below:
Developing a mental health and psychosocial support (MHPSS) package for infectious disease outbreaks

Credit: Egyptian Red Crescent A collaboration between UK-PHRST and Saint Joseph University of Beirut, this research project aims to identify, through expert consensus, a list of interventions to support people’s mental and psychosocial health as part of a complex package for an infectious disease outbreak context.
As part of this project, a consultation workshop was held in Cairo, Egypt from 8-10 May 2023 hosted by the Egyptian Red Crescent (ERC). Participants, including people with lived experience from the Global Mental Health Peer Network, shared their experiences of mental health and psychosocial support (MHPSS), and experts identified barriers and facilitators for MHPSS in outbreaks. The workshop provided valuable learning allowing the project team to focus on developing MHPSS priorities with country partners.
Epidemiological and clinical review of mpox in Nigeria: A multi-disciplinary research project to inform outbreak control measures (with Nigeria CDC)
The UK-PHRST team continue to collaborate with Nigeria CDC to develop two interlocking research studies. Using a OneHealth approach, the project aims to better understand the factors behind the spread of mpox across different Nigerian states.
A UK-PHRST research team travelled to Abuja in May to finalise project details prior to the study implementation later this year. Researchers from the UK-PHRST, including colleagues from the University of Oxford also assisted Nigeria CDC colleagues to further strengthen their laboratory systems ahead of the studies. For instance, one workshop provided attendees with hands-on experience of preparing, running and analysing blood sample analysis assays as well as the transfer of scientific methods to build local skills capacity for the upcoming studies.Completed research projects
New briefing paper flags priority research questions to improve cleaning practices in resource-limited hospital settings
The CLEAN research group, first convened in mid-2022 within a UK-PHRST project, have produced a briefing report that outlines the need for additional research work in the field of environmental cleaning in resource-limited healthcare settings. The report details their 12 recommended key research questions and associated considerations to facilitate effective hospital cleaning in resource-limited healthcare settings and to help reduce the spread of infections and antimicrobial resistance.
They hope the research priorities will encourage the eventual implementation of low-resource tailored and cost-effective cleaning practices in resource-limited settings which will benefit the health of both patients and staff and ensure a respectful environment for patients. They are now calling on funders, policymakers and advocates to drive forward implementation research into cleaning practices in these healthcare settings.
Operational research framework workshop at Africa CDC
March - Members of the research team supported the facilitation of a consultative workshop held in Addis Ababa on developing an operational research framework in emergency preparedness and response at Africa CDC. The workshop built on remote support provided by the research team in developing the concept, format and agenda in previous months. The team will continue to support Africa CDC as the framework develops.
- Read more

Credit: Louis Leeson LSHTM Cleaners must be viewed as a key part of the health system to reduce infections and antimicrobial resistance among staff and patients, according to a report by experts from the CLEAN research group.
The group produced the briefing paper as part of a UK-PHRST project. It sets out 12 priority research questions to improve hospital cleaning and highlights the challenges facing resource-limited settings, as well as factors that need to be considered to support the implementation of tailored and effective cleaning practices. These include, for example, ensuring capacity strengthening of cleaners and the need for financial support to cement cleaning in the healthcare system.
The Group is now calling on investors, policymakers and advocates to drive forward implementation research into cleaning practices in hospitals with limited resources.
The CLEAN Group was first convened in mid-2022 within a UK-PHRST project to identify the most urgent research questions to inform or enhance the implementation of best practices in surface and non-critical equipment cleaning in healthcare facilities in resource-limited settings. It includes experts from Africa, Europe, Asia, Australia, North and South America, with expertise in infection prevention and control, hospital cleaning and disinfection, water, sanitation and hygiene (WASH), health policy, implementation science and clinical research in resource-limited settings.
Read the full blog and the CLEAN Briefing Paper on the UK-PHRST Knowledge Hub.
- Read more
The UK Public Health Rapid Support Team invites you to join our new drive to evaluate the definition, value and impact of our partnerships and capacity strengthening activities.
Fill out our Market Consultation Survey to indicate your interest in the competition to receive a contract. The contract will involve conducting the evaluation and generating significant learning and understanding of our partners' perspectives, identifying challenges and how these have and can be addressed in real time over the lifespan of UK-PHRST's project cycle.
Some key considerations for the evaluation include:
Partnerships
- Understanding of the "nuance of relationship" by different partners
- The degree to which they are perceived as beneficial and equitable by the people we work with
- What factors appear to enable or detract from "ideal partnerships" –what does the much-used phrase "power dynamics" mean in our context?
- Is it constraining in crafting equitable and useful partnerships?
- Does it play a facilitative role, or is it neutral in its perception by partners?
- What impacts have our partnerships had?
Capacity strengthening
- How can we gauge a deeper understanding of capacity strengthening in the context of UK-PHRST's work?
- What are the impacts realised by partners in their work with the UK-PHRST?
Information session
For more information, please join us online at our Market Engagement Session on 15 December 2022 at 10:00 am GMT. Join here
In order to be considered, please complete the Market Consultation Survey here.
This should be completed by the supplier or a partner or an authorised representative in his / her own name and on behalf of the company / organisation completing this questionnaire.Registration is free and open to all. The deadline to complete the survey is 13 January 2023.
More information
Find out moreFor further information, please refer to the documents attached, including:
download Attachment 2 - How to Bid including Evaluation Criteria v1.0.pdf
download Attachment 1 - About the Procurement Competition v1.0.pdf
download Market Consultation Survey - Evaluation of UK-PHRST Partnerships Capacity.docx
download Pre-sourcing event Zoom meeting invite link.docx
Please contact [email protected] if you have any questions.
- Read more
The UK Public Health Rapid Support Team and partners are currently working on seven research projects, and we have also developed our Research Plan for 2022-2025. Within the plan, we have described 17 new cross-discipline research projects that were co-identified and will be co-led with low-and-middle income partners, and three of these have recently started. Projects in the plan have been grouped into themes covering preparedness and prevention, detection, response, and impact and evaluation, however, the plan also enables flexibility to begin new projects that address urgent research questions arising during outbreaks or during deployments. Most of the 14 projects yet to be approved by Technical Steering Committee (TSC) are expected to be reviewed and begin over the next six months.
We are also delighted to announce a new research collaboration on Monkeypox with the Nigeria Centre for Disease Control, University of Oxford and partners. This new collaboration will cover key priorities in Monkeypox research in Nigeria and will have clinical, epidemiological, One Health, laboratory, and social science components. Priorities for the Monkeypox research programme were identified during a workshop in Abuja in August 2022, during which participants proposed several multi-disciplinary studies with Nigerian leads. The group also recommended strengthening laboratory operations at Nigeria CDC in preparation for the research, and this work is currently underway. The Monkeypox research programme is included in our research plan.
Among our currently running studies, one is developing an early warning system that can identify “hot spots” in remote regions of Guinea where Marburg virus outbreaks are likely, based on interactions between human and bat populations. In recent months, the study team have completed a community sensitisation (awareness raising) and a risk communication campaign across study villages in Macenta, led by the Guinean project lead in collaboration with a local NGO. They have also collected pilot data for surveillance tools from study villages and generated preliminary biodiversity indicators and machine learning algorithms. The next stage of the project will include in-depth investigations of zoonotic exposure and bushmeat hunting practises among the target population using qualitative methods.
Since the last research update, three research projects have been completed, including two Infection Prevention and Control (IPC) studies and a pilot study of a non-whole genome sequencing approach for monitoring SARS-CoV-2 variants in Burkina and Kenya. Find out more below.
Development and evaluation of resources to support IPC engagement with caregivers in hospitals
This study, which began in February 2021, aimed to develop and evaluate resources to support informal caregivers in Cameroon to engage with IPC . The project was co-led by the UK-PHRST and Cameroon Baptist Convention Health Services (CBCHS) in partnership with the Infection Control Africa Network (ICAN), the not-for-profit visual resource charity Medical Aid Films (MAF) and the Africa Task Force for Corona Virus Response (AFTCOR) IPC technical working group.
Thee study described the role and function of caregivers in a tertiary referral hospital in Cameroon, developed training resources to support their engagement with IPC, including context-appropriate audio-visual materials, piloted delivery of a multimodal intervention, and evaluated the effectiveness of the intervention.
The evaluation demonstrated the feasibility of delivering the intervention in the health system and that it was well-received by caregivers and health workers. Six local research assistants were also trained. The study findings have been and are being shared with all relevant stakeholders, including ICAN, MAF, Africa Centres for Disease Control and Prevention (Africa CDC), and the Cameroon Public Health Institute. The study team plans to present the findings at the bi-annual ICAN conference in 2023 via partner networks and in an open access, peer reviewed journal. The team will support further engagement of informal caregivers with a ‘toolkit’ of resources that will be transferable to other LMIC healthcare settings.
What is the current level of cleaning in LMIC health systems and what interventions are effective at improving it?
Formal training for cleaners in health settings may be inadequate in many LMICs and is of particular concern during outbreaks when there is additional urgency for rapid interventions.
In this study, the team led a systematic review of cleaning interventions in LMIC health settings and convened a workshop with diverse international stakeholders to develop recommendations and a roadmap of future research priorities. Stakeholders included leading IPC researchers in Africa, Asia and high-income countries, and representatives from public health institutes, relevant networks and the World Health Organization.
Unsurprisingly, most evidence from LMICs came from areas with greater resources, such as tertiary referral centres in large cities. Standard outcome definitions for cleanliness were found to be lacking, and results were reported inconsistently, hampering the synthesis and meta-analysis of aggregate data. Preliminary systematic review findings have been presented in a Webber teleclass and are being submitted for presentation to the ICAN conference and International Conference on Infection Prevention and Control in 2023. A blog and research prioritisation paper have been submitted to The Global Health Network, and the systematic review will be submitted for publication in a peer-reviewed journal.
A non-whole genome sequencing approach for monitoring SARS-CoV-2 variants in Burkina Faso and Kenya
This study, which started in November 2021 and was a collaboration between UK-PHRST/LSHTM and Groupe de Recherche-Action en Santé in Burkina Faso (GRAS), Kenya Medical Research Institute (KEMRI), MRC Unit Gambia (MRCG) and Liverpool School of Tropical Medicine (LSTM), aimed to understand the feasibility of running the HRM assay in LMIC settings through pilots in Burkina Faso and Kenya. These sites were selected because the research team had established partnerships through the Gates Foundation-funded Malaria as a Risk Factor for COVID-19 (MALCOV) SStudy. UK-PHRST Rapid Research funding enabled the team to leverage real-time access to MALCOV study specimens.
The study team developed and updated their high-resolution melt (HRM) assay in response to the emergence of new SARS-CoV-2 VOCs. Following training, researchers from Burkina Faso and Kenya analysed samples using the assay at laboratories in The Gambia and Kenya and validated assay performance against whole genome sequencing (WGS). This project demonstrated the utility of a non-WGS method in lower resource settings for tracking SARS-CoV-2 variants and may provide a lower-cost approach for understanding molecular epidemiology in settings where access to WGS is absent or limited. The project built new and developed existing collaborative working relationships between researchers from LSHTM, Groupe de Recherche Action Santé (GRAS), Kenya Medical Research Institute (KEMRI), MRC Unit The Gambia at LSHTM (MRCG) and Liverpool School of Tropical Medicine (LSTM). The findings have been presented at LSHTM and external meetings and conferences. One peer-reviewed article is nearing publication in the Scientific Reports journal, and a further article will be submitted in December 2022. Find out more about the field visit to The Gambia here.
- Read more
In the coming months, the UK Public Health Rapid Support Team (UK-PHRST) will focus on establishing a refreshed and enhanced capacity strengthening pillar. Dr Claire Bayntun has been appointed to lead this work as the Head of Capacity Strengthening and will expand the team to take forward new strategic spheres of opportunities, reflecting the values of the UK-PHRST and aiming to secure trusted, sustainable partnerships for the future.
View UK-PHRST's capacity strengthening pillar
Over the last quarter, the UK Public Health Rapid Support Team (UK-PHRST) conducted eight capacity strengthening activities, including a learning review in Cape Town, South Africa, and R training* in Ethiopia and Nigeria, respectively.
*R is an open-source software environment for statistical computing and is used for data analysis and visualisation.In September, we met with many of our partners in Cape Town, South Africa, to reflect on our working practices and exchange lessons on improving outbreak response, research and capacity strengthening. Experts at UK-PHRST co-led sessions on gender equity, capacity strengthening, policy and practice in research, outbreak response and equitable partnerships. These discussions will inform a summary of recommendations and actions we can implement to enhance our equitable partnerships and foster sustainable ways of working.
Watch the highlights of the learning review
R Training
UK-PHRST facilitated R-Training with Africa Centre for Disease Control and Prevention in Ethiopia in July, capturing lessons learned to strengthen future training, planning and delivery. The UK-PHRST epidemiology team co-facilitated two workshops with the African Volunteer Health Corps (AVoHC). This included prioritising key programme activities for 2022-23, reviewing and refining content for an induction course, and training new AVoHC roster members.
Equitable partnerships with infection prevention and control (IPC) stakeholders
The infection prevention and control (IPC) team shared preliminary results for developing and evaluating resources to support a study with Cameroonian partners in July. It delivered a workshop with key global stakeholders reviewing evidence and prioritising research needs for cleaning and disinfection interventions.
The team is contributing to reviewing a World Health Organization course for environmental cleaning and infection prevention control. The team is supporting the WHO Emergencies IPC team, offering technical support for Ebola and Monkeypox, and developing specific IPC implementation tools, including an IPC outbreak implementation package and updated IPC assessment tools will be provided in addition.
Mental health
As part of the Strengthening Public Mental Health in Africa in response to COVID-19 (SPACE) programme’s phase two delivery, the team involved representatives from Sierra Leone and Cameroon in a workshop in Liberia with partners Africa Centre for Disease Control, World Health Organization Regional Office for Africa (WHO AFRO), WHO Regional Office for the Eastern Mediterranean (WHO EMRO), West Africa Health Organisation (WAHO), and East Central and Southern Africa Health Community (ECSA-HC).
- Read more
We have summarised the latest UK-PHRST deployment, research and capacity development activities from July – September 2022 in a quarterly map. Many of our activities across the triple remit overlap, and some will continue into the next quarter. The map demonstrates ongoing or completed activities during the quarter, and the year stated is when the project commenced.
- Read more
The Strategic Framework 2022 to 2025 sets out UK-PHRST’s objectives to build on the commitment, impact and effectiveness of the past six years of our operations.
The UK-PHRST strategy is underpinned by three principles: learning, partnerships and impact. It outlines how the UK-PHRST will deliver on this commitment through activities across the triple remit in outbreak response, research and capacity strengthening.
- Read more
On the week that the UK Public Health Rapid Support Team (UK-PHRST) celebrates its 6th sixth year anniversary, and with staff currently deployed to the Ebola outbreak in Uganda, UK-PHRST Director, Dr Ed Newman, shares the team’s ambitions for the next three years and our continued commitment to respond to disease outbreaks in the countries we work with.
Published by the UK Health Security Agency. Read more.
We are an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine, funded with UK aid by the UK Department of Health and Social Care.
- Read more
In celebration of World Field Epidemiology Day on 7 September, the UK Public Health Rapid Support Team spoke to UK Field Epidemiology Training Program (UK-FETP) fellows Megan Bardsley and Mona Dave, who recently deployed with the UK Public Health Rapid Support Team (UK-PHRST). Field epidemiologists support the UK-PHRST to prevent and control infectious disease outbreaks, before they develop into global emergencies. The UK Field Epidemiology Training Programme recruits seven to eight UK-FETP fellows a year.
Megan Bardsley

Megan completed her undergraduate degree in biological sciences and studied an MSc in Control of Infectious Diseases at the London School of Hygiene & Tropical Medicine. She is in her second year of the Field Epidemiology Training Programme based in Field Service South West with the UK Health Security Agency (UKHSA). Before joining UK-FETP, she had prior experience in UKHSA’s human immunodeficiency virus / sexually transmitted infections (HIV/STI) department, worked as a research assistant at LSHTM and gained experience in Malaysia at a breastfeeding NGO. She recently deployed with UK-PHRST to Papua New Guinea via the Global Outbreak Alert and Response Network.
Mona Dave

Mona gained an undergraduate degree in biomedical sciences at Warwick University, and a Master's in Public Health with International Health at the University of Nottingham. She began her journey into global health after spending three months in the Philippines on a health education programme with the Voluntary Service Overseas (VSO) as part of the International Citizen Service (ICS) in 2013. Before joining the UK-FETP, she worked as a research assistant in non-communicable disease research at Newcastle University and as a scientist in the South West Field Service. Mona recently deployed with UK-PHRST and is currently based at a training site at UKHSA's Midlands Field Service.
What is epidemiology?
How do epidemiologists contribute to outbreak response?
Megan: Responding to an outbreak of disease in epidemiology involves providing and interpreting data to understand the severity of the situation, affected groups, what people are being infected by, and the impact and burden. You then highlight particular risk factors and groups that need targeting for intervention. One key role of the epidemiologist in an outbreak is getting everybody to agree on the case definition.
Mona: Contributing to regular disease surveillance allows us to understand 'normal' patterns and trends of disease spread. In other words, we can spot, investigate, and act when something looks out of the ordinary. Descriptive epidemiology (describing a disease in time, person and place) and analytical epidemiology (conducting statistical analysis to test a hypothesis) can explain how an infection might spread. However, you may not always know the true cause. As an epidemiologist, being able to interpret findings, make evidence-based recommendations and tailor these to your audience can help to ensure recommendations are actioned by the right stakeholders and, therefore, control further infections from spreading.
What does the role involve?
Megan: It involves working with many different people and using your technical expertise and scientific background to identify trends in surveillance data and present the strengths and limitations to various stakeholders. When investigating a public health outbreak, I am responsible for managing the data, writing code to analyse the data, and working with people to identify and describe cases and do detective work to investigate the source.
Mona: I support UKHSA's Midlands Field Service infectious disease surveillance and outbreak response work as part of a rota. This can involve producing or reviewing epidemiological summaries, attending outbreak control meetings and providing feedback and recommendations. I also work on specific projects that enable me to enhance existing and develop new skills while meeting my UK-FETP competencies.
What is a highlight of your job?
Megan: I worked on an investigation into an outbreak of Salmonella where I rang patients to complete questionnaires and conducted an analytical study, also known as a case-control study. Secondly, I enjoy being part of a global epidemiology network - it's a community of people who are interested in the spread of infectious diseases and you learn from people across the world.
What challenges do you experience in your role?
Megan: I think a lack of awareness of epidemiology can be challenging as some of the fantastic work we produce can go unacknowledged. I think increased awareness of epidemiology will attract more people who are interested in helping people through the use of science.
What led you to apply for UK-FETP?
Mona: As challenging as it was, contributing to the COVID-19 response, seeing the impact and working alongside dedicated individuals is incredibly rewarding. That was when I realised I wanted to continue working in and developing my skills in this field, and I applied for the UK Field Epidemiology Training Programme (UK-FETP).About UK-FETP
The United Kingdom Field Epidemiology Training Program (UK-FETP) was founded in 2011 as a program associated with the European Program for Intervention Epidemiology Training (EPIET), and it was accredited by TEPHINET in the first accreditation round. Since EU-Exit the UKFETP has run as an independent programme for the UK.
About UK-PHRST
The UK-PHRST is an innovative partnership between the UK Health Security Agency and the London School of Hygiene & Tropical Medicine, funded with UK aid by the UK Department of Health and Social Care.
- Read more
The UK Public Health Rapid Support Team (UK-PHRST) and partners are currently delivering nine research projects, including two new studies bolstering UK-PHRST's research in outbreak preparedness and response:
- 'A novel One Health approach to develop an early warning system to improve preparedness for and response to Marburg virus disease outbreaks'. This innovative study combines serological sampling of humans and Marburg virus detection from faecal bat samples to confirm target populations and uses remote audio-monitoring devices (AudioMoth) to assess humans and bat population interaction in target regions in Guinea. The team will use these findings to develop an early warning system to allow public health systems to recognise MARV outbreak threats with greater precision and prepare response measures tailored to affected areas. The study is being co-delivered with University of Oxford, the National Viral Haemorrhagic Fever Reference Laboratory, Guinea and MRC Unit The Gambia at the London School of Hygiene & Tropical Medicine (LSHTM).
- 'A novel early warning system involving local community leaders for early detection of health-related events indicative of outbreaks: A pilot in Cape Verde and Brazil'. This project, a collaboration between Brasília University, the Ministry of Health in Cape Verde and the UK-PHRST, investigates whether an event based surveillance (EBS) system - developed with and relying on the participation of community leaders - is more effective at detecting infectious disease outbreaks than indicator-based surveillance or centralised EBS systems. The study team will focus on two contrasting outbreak prone lower middle-income countries (LMICs), Cape Verde and Brazil, respectively.
In other active studies in the UK-PHRST portfolio, the project team delivering a pilot of a non-whole genome sequencing approach for monitoring SARS-CoV-2 variants in Burkina Faso conducted a successful research and laboratory visit to MRC Gambia Unit The Gambia at LSHTM in July 2022. See further details of the visit. The team had needed to move sequencing and assay development to two new sites, at MRC Gambia and Kenya, following a coup in Burkina Faso earlier in the year. The project team will submit a final report in October.
The study 'Rapid response molecular diagnostics for Crimean-Congo Haemorrhagic Fever (CCHF)', which aims to assist the economic development and welfare of CCHF endemic populations in LMICs, particularly those in marginalised areas with limited laboratory capacity, conducted its final visit to the Ministry of Health virology laboratory in Turkey in June 2022. A UK-PHRST-hosted CCHF workshop in September 2022 is in preparation to disseminate results to key stakeholders.
The UK-PHRST also convened a two day hybrid research workshop in June 2022 in partnership with Stellenbosch University as part of the UK-PRHST study investigating 'evidence on levels of, and interventions to improve, healthcare cleaning in low-and middle-income countries. Over 30 regional and international organisations attended, including experts in water, sanitation and hygiene (WASH), Infection prevention and control (IPC) and environmental hygiene. A report and roadmap are currently in preparation and will be published in due course as outputs.
A closing ceremony for the IPC Caregivers study in Cameroon, which focused on the development and evaluation of resources to support IPC engagement with caregivers in LMIC hospitals, was held at Banso Hospital on 24 June 2022 to mark the contribution of the research team and the conclusion of field research. As part of the study, a series of IPC instructional/orientation animated videos were developed in partnership with Medical Aid Films and designed for caregivers of patients. See the animations in English and in Pidgin. A short version of the film was also produced. The project team are writing the final project report currently, and will also present findings within the Infection Control Africa Network (ICAN) webinar series and at the upcoming Global Health Network Conference.
Three research projects have also been completed since the last research update. These include the study which examined excess mortalities associated with COVID-19 in The Gambia, as well as two rapid studies; one to improve the application of oral fluid filovirus surveillance methods in Africa, and one focused on the development of mental health and psychosocial support (MHPSS) in outbreak preparedness and response in Africa.
The study team investigating excess mortality in The Gambia associated with COVID-19 and other causes concluded there was an unexpected decline in recorded mortality during the COVID-19 pandemic, but that mortality rates increased in the second wave and reached excess mortality of 22.6 per 100,000 compared to 2016-2019. Foetal complications constituted the highest proportion of deaths, while sepsis, COVID-19 and stroke were also important. A report written by UK-PHRST, MRC Unit The Gambia at LSHTM and Ministry of Health Gambia has been shared with regional health centres and health facilities participating in the study. Results will also be disseminated through a policy briefing, Ministry of Health meetings, and presentations at national and regional meetings.
The second completed study, conducted in partnership with University of Oxford and the Fondation sante et développement durable (FOSAD) Guinea, set out to understand if the Lola population in Guinea exhibited signatures indicative of non-Ebola filovirus infections that impact upon individual and population-level seroepidemiological inference, and if so, if this information could be used to refine strategies for both oral fluid and serum-based seroepidemiological investigations in filovirus-endemic LMICs in Africa. The study demonstrated that oral fluid samples showed discordant responses with blood and concluded that at population scale, and despite prior validation of the assay in an Ebola virus survivor cohort, surveillance for Ebola virus and likely other filoviruses appeared unfeasible with oral fluid-based assays due to insufficient specificity. These limitations are important for public health professionals and researchers using oral fluid tools for the surveillance of filoviruses as they were widely used during and after the outbreak of Ebola in West Africa and have been suggested as more acceptable tools for surveillance in endemic settings. Results from the study were disseminated in Guinea through the national health security agency (ANSS), who lead operations and research strategy related to emerging infectious diseases including filoviruses. The study highlights the limitations of relying on oral fluid based surveillance for filoviruses and suggest dried blood spot (DBS) based sampling as a viable alternative.
The study ‘Evidence to practice: research and capacity development for mental health and psychosocial support (MHPSS) in outbreak preparedness and response in Africa: SPACE 2.0’, sought to support national actors in Liberia, Sierra Leone, Cameroon and Nigeria prone to outbreaks to integrate mental health interventions in emergency preparedness and response (EPR). An umbrella review on the effectiveness of mental health and psychosocial support (MHPSS) interventions during infectious disease outbreaks was conducted, and a hybrid workshop was held in Liberia which brought together mental health experts from African public health institutions. This included World Health Organization Regional Office for Africa (WHO Afro), Africa Centres for Disease Control and Prevention (Africa CDC), West African Health Organization (WAHO), East, Central and Southern Africa Health Community (ECSA-HC) and mental health leaders in Liberia, Sierra Leone, Cameroon, and Nigeria to share expertise and develop a theory of change (ToC) for integrating mental health into national EPR plans. Capacity building activities included introducing the newly developed Minimum Services Package for MHPSS in emergency response, and related MHPSS resources. The UK-PHRST mental health consortium convened a further webinar on 18 May 2022 at which results from the study were shared, and next steps discussed, including:
- How best to facilitate sharing expertise and lessons learned from different countries responses to the COVID-19 pandemic and other emergencies
- How to further improve and refine the ToC for MHPSS integration into emergency response
- Identification of research and capacity strengthening priorities for the next phase of the consortium’s work.
- 'A novel One Health approach to develop an early warning system to improve preparedness for and response to Marburg virus disease outbreaks'. This innovative study combines serological sampling of humans and Marburg virus detection from faecal bat samples to confirm target populations and uses remote audio-monitoring devices (AudioMoth) to assess humans and bat population interaction in target regions in Guinea. The team will use these findings to develop an early warning system to allow public health systems to recognise MARV outbreak threats with greater precision and prepare response measures tailored to affected areas. The study is being co-delivered with University of Oxford, the National Viral Haemorrhagic Fever Reference Laboratory, Guinea and MRC Unit The Gambia at the London School of Hygiene & Tropical Medicine (LSHTM).
- Read more
We have summarised the latest UK-PHRST deployment, research and capacity development activities from April – June 2022 in a quarterly map. Many of our activities across the triple remit overlap, and some will continue into the next quarter. The map demonstrates ongoing or completed activities during the quarter, and the year stated is when the project commenced.
View the UK-PHRST quarterly map
- Read more
The UK-PHRST team and partners are currently delivering 11 research projects, including two new studies:
- ‘Integrating Social Science into Africa CDC’s Public Health Operations’, which examines the status and use of social science at Africa CDC and how it can be further integrated into public health preparedness and response.
- ‘What is the current level of cleaning in LMIC health systems and what interventions are effective at improving it?’ which strengthens UK-PHRST's research in Infection Prevention and Control (IPC) and environmental hygiene and aims to improve the evidence base for cleaning implementation and investment in cleaners, a vulnerable and neglected group in the health system in many Lower Middle-Income Countries (LMICs).
We are also delighted to welcome Nasser Fardousi to the UK-PHRST, who joined us as a Research Fellow in Environmental Hygiene in January. Nasser is working with the IPC team, investigating the current level of cleaning in LMIC health systems and what interventions are effective at improving it.
We have several research projects that are concluding. These include two rapid research studies, one of which aims to improve the application of oral fluid filovirus surveillance methods in Africa, and the other to develop mental health and psychosocial support (MHPSS) in outbreak preparedness and response in Africa. The team investigating the extent of excess mortality in health facilities in The Gambia associated with the COVID-19 pandemic is also in the final stages of writing up their results.
In February, as part of the MHPSS study, the team delivered a workshop in Liberia in partnership with Africa CDC hosted by the Liberian Ministry of Health. The workshop brought together a consortium of mental health experts from African public health institutions to share experiences and lessons learned from COVID-19 and other crises in the region. The workshop also mapped out processes for strengthening MHPSS in outbreak preparedness and response in Africa.
A military Coup in Burkina Faso in January 2022 threatened to affect the delivery of the rapid study piloting a non-whole genome sequencing approach for monitoring SARS-CoV-2 variants in Burkina Faso, however, the team were able to move sequencing and assay development to The MRC Unit The Gambia at the London School of Hygiene & Tropical Medicine and a new field site in Kenya.
Our study on COVID-19 vaccine strategies implementation in partnership with Gates Exemplars in Global Health has been published online and will soon be published in French. Read more here.
The research management team are also preparing the programme’s six-month report for National Institute for Health and Care Research (NIHR), including quarterly and annual finance reports.
Our newly developed research strategy for 2022-2025 is currently in review by our key stakeholders. The strategy has been informed by an evidence gap analysis complemented by stakeholder interviews and feedback from partners and formal reviews and aims to deliver a coherent, structured, partner-led research programme informed by public health need.
- ‘Integrating Social Science into Africa CDC’s Public Health Operations’, which examines the status and use of social science at Africa CDC and how it can be further integrated into public health preparedness and response.




Responding effectively to outbreaks of infectious diseases saves lives. Sharing knowledge, learning, and experience of outbreak response across geographies, diseases, and between researchers and policy makers is essential. Without collaboration, outbreaks risk spreading in size and scale.
The UK-PHRST are pleased to share their Global Health Network Knowledge Hub, where practitioners and researchers can find and share the most useful information for their work in outbreak response.
Hosted on The Global Health Network, the Knowledge Hub aims to:
- Bridge the gap between the fast-paced world of online discussion forums and maintain long-term access to useful resources.
- Share up-to-date research and policy, as well as a dedicated education and training area with resources to support learning and inform effective outbreak response.
- Connect UK-based researchers with specialists in LMICs, creating a flow of information exchange and localised adaptations to outbreaks.
Many of these resources have been developed by UK-PHRST and its partners.
- About The Global Health Network
Faster and better research is critical to solving the world’s biggest health challenges. The Global Health Network enables researchers and institutions to share best practice and know-how with each other to drive progress, while empowering local health professionals undertaking research in the world’s most vulnerable settings. The Global Health Network facilitates sustainable health improvements through sharing of research methods, knowledge and experience through an open-access online platform and face-to-face within varied healthcare settings. It delivers training, skills and career development to frontline health workers, no matter where they are or how resource-constrained their environment may be. The result is easier, faster, better research to help address the world's biggest health challenges.
Visit: www.theglobalhealthnetwork.org.
The UK-PHRST are deployed to outbreaks all over the world from Bangladesh to Nigeria to Sudan. Working alongside in-country staff from Minstries of Health, NGOs and other government organisations, UK-PHRST successfully help combat the outbreak and protect against future threats to health. Read some of our stories below.
If you're interested in more technical case studies, diving deeper into the UK-PHRST's approach to its work, visit our Global Health Network page.
- Using PPE in outbreak response
The UK Public Health Rapid Support Team (UK-PHRST), funded by UK aid from the Department of Health and Social Care, supports low- and middle-income countries in investigating and responding to disease outbreaks and conducts research to improve our response to future epidemics.
Our expertise in infection and prevention and control, which includes the use of Personal Protective Equipment (PPE), is used to protect people from infection in disease outbreaks. PPE can diminish transmission when used as part of an integrated package of measures, and crucially helps protect medical staff from disease, but there is variation in the need for, and use of PPE for different diseases, across countries, and differing views on its necessity.
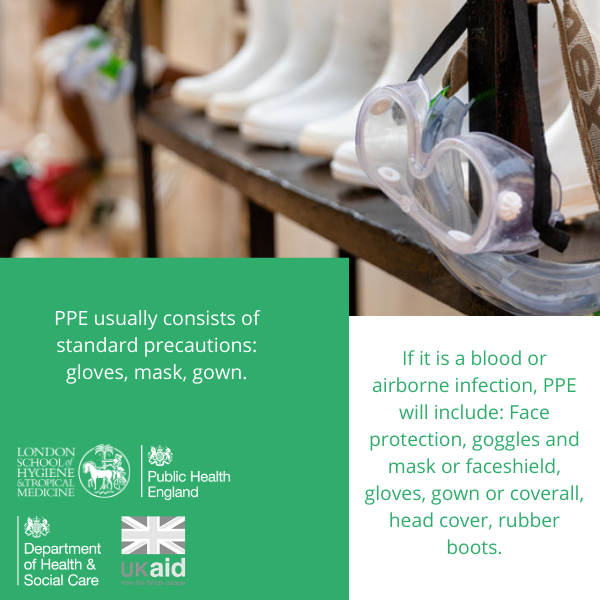
This project investigated the use of PPE to protect people from Lassa Fever, in specific Lassa Fever Treatment Centres (LTCs) across Nigeria.
Lassa fever is often confused with Ebola or other viral haemorrhagic fevers, but it differs - it is less fatal, and its transmission is very different. Ebola is transmitted between people, whereas Lassa fever is spread to most people (~80%) through exposure to food or household items contaminated by rats. Less commonly, transmission can occur in laboratories, or between people, particularly in health care settings with inadequate infection prevention and control measures.
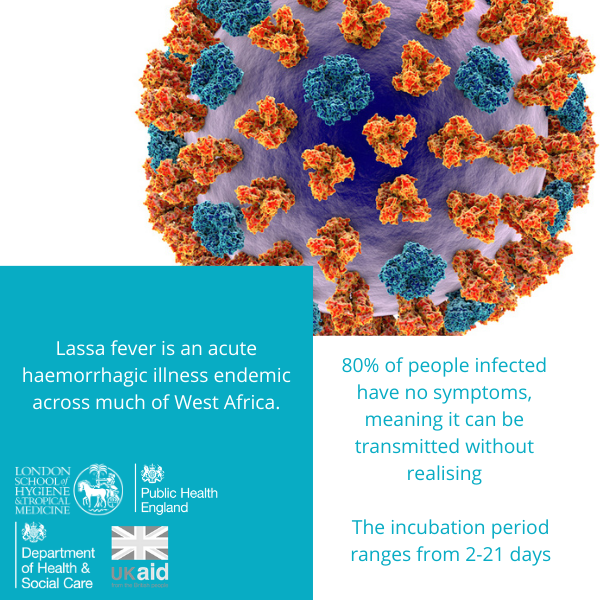
Why are the UK-PHRST involved?
Lassa Fever is an important cause of outbreaks of infectious disease. It is one of the pathogens in the World Health Organizations’ list of epidemic threats needing urgent research. The disease is endemic in rodent populations in parts of West Africa including Benin, Ghana, Guinea, Liberia, Mali, Sierra Leone, Togo, and Nigeria, and most likely exists in other West African countries as well. Cases are increasing in Nigeria.The nuances between viruses causing haemorrhagic fevers, such as Ebola and Lassa Fever, are not translated into official guidance, and policies end up addressing them in the same manner. In addition, much of the research and guidance for PPE are developed in high-income settings, where there are few cases of disease, therefore the guidance is built on data, rather than lived experience.
Recognising limitations in existing guidance, The Nigerian Centre for Disease Control (NCDC) invited the UK-PHRST work with them to investigate whether their infection, prevention and control (IPC) policies devised in 2017 were effectively disseminated and how, in the case of Lassa Fever, they were operationalised.

A woman suspected of contracting Lassa Fever awaits her lab results in quarantine. Suspect cases of Lassa Fever typically wait 12-24 hours for their samples to be tested locally at the virology laboratory. If positive they are moved by ambulance to the confirmed case ward a short distance away. What did they discover?
The team found that health care workers in Lassa treatment centres (LTCs) were frequently not using PPE in line with government guidelines. Limited availability of PPE in some centres led to health care workers using personal risk assessments to drive decision-making about its use, and there is a gap in understanding of staff perceptions, and how they protect themselves, in the absence of adequate PPE.
During interviews, researchers noticed that much importance was placed on the language, behaviour and understanding of PPE by the health workers. For example, some staff were basing their decision-making on what they perceived as ‘careful’ best practice, but this is not reflected in guidance. Staff also consistently expressed challenges with using PPE, for example in the environment they were using it in (high temperatures), with poor quality materials (gloves breaking or tearing), and limited function (reduced visibility when using eye protection).

Inside the grounds of the Federal Training Hospital (FETHA) in Abakaliki, a makeshift Lassa Fever holding centre is prepared for quarantining of suspected cases. To mitigate some of these issues, some health workers adapted PPE to suit their local context; for example, choosing to wear a surgical gown in replacement of gowns provided, saying they were cooler to wear and simpler to remove.
The study team observed that judgements made by health workers were based on their experience and understanding of the situation, and this was very different to PPE guidance from international and national bodies.

Demonstrating a correctly prepared personal protective equipment suit In low- and middle-income countries (LMICs), funds assigned for PPE procurement and supplies can be limited. Where there are competing demands, funds are often redirected to more immediate requirements, such as emergency operations, or treatments.
Alongside this, there were worries that the PPE provided was substandard. Much of the PPE in use had been donated, for example from non-governmental organisations, and there was no formal process in place to ensure it was fit for purpose.
Capacity building: Preventing future fires
As a result of the collaborative work carried out in the LTCs, The Nigeria Centre for Disease Control (NCDC) has revised national guidance on infection prevention control for viral haemorrhagic fevers.
Together with this success, emphasis on the quality of PPE facilitated prompted dialogue at a national level about developing assurance systems so that donation of equipment is fit for purpose in the future. These results have informed national advocacy work for improvements to supplies to Lassa Treatment Centres – with the ultimate aim of reducing countrywide infection.

Dr Abdulmajid Suleiman Musa shows a group of NCDC staff how a correctly prepared PPE suit should look when working in a virus hit region, Keffi, Nasarawa state. 
Nurse Mary Obasi measures the temperature of woman with Lassa Fever in the confirmed ward at the FETHA 02 facility, Abakaliki, Ebonyi state How can this work be translated into other contexts?
There has also been ongoing professional collaboration between the NCDC as part of the COVID-19 response with Africa Centre for Disease Control and as part of the African Union Taskforce for COVID-19.
Thinking through novel and more nuanced approaches to PPE is useful when considering PPE for COVID-19. It is also helpful in the face of supply chain issues, with many countries unable to source PPE during the pandemic. Rational use of PPE has been suggested to mitigate insufficient PPE supplies.
While COVID-19 has brought worldwide disruptions to PPE supplies, and its availability, the experience of clinicians in LMICs has much to teach us all about the realities of working with limited resources; developing adaptations and creating innovative local solutions. However, it is important that guidelines are rooted in evidence-based best practise, as well as reflecting the reality of those who are required to implement them.
Read the updated guidelines and vital role the NCDC plays in keeping hospitals, clinics, and health facilities safe and free from disease.
- Deploying our Rapid Response Mobile Lab into the heart of disease outbreaks

Image credits: WHO Europe What is a Rapid Response Mobile Lab?
Rapid Response Mobile Labs (RRMLs) bring critical laboratory resources and diagnostic surge capability to the doorstep of affected and vulnerable communities, often in hard-to reach remote areas during outbreaks. Staffed by expert scientists, RRMLs come in one of five main functional set ups, from a highly compact single case unit to a full-scale self-contained laboratory truck.
They are highly adaptable based on the context they need to be used in - boosting local diagnostic capacity for a National Public Health service disrupted during a crisis, providing surge diagnostics capacity at the epicentre of an outbreak or supporting disease surveillance and research.
Since regular deployments started in the early 2000s, mobile labs providing diagnostics in the field have been a central part of managing outbreaks of diseases such as viral haemorrhagic fever. During the 2014-2016 Ebola outbreak, deployments like European Mobile Laboratory (EMLab) Project reduced sample-to-result turnaround times from days to hours, increasing the effectiveness of the response to the epidemic.
Using the Rapid Response Mobile Lab for UK-PHRST's research, capacity strengthening and outbreak response activities
The UK-PHRST microbiology team operate a “Type II” RRML set up, consisting of several robust flight cases that can be easily transported by van or aircraft, allowing our experts to respond to outbreaks in remote locations. The RRML adapts its function to each unique situation –from identifying unknown pathogens to tracking the spread of an outbreak following natural disasters or mass migration events.
When no diagnostic capability exists, the RRML can be deployed straight into the centre of the outbreak, substantially reducing test turnaround times. Where some diagnostic capacity exists, such as in hospital labs or National Public Health Institutes, the RRML can provide ‘surge’ testing capacity to bolster this further by increasing the number of tests that be conducted per day, or by increasing the range of tests available.
The RRML can also add value during humanitarian crises by supporting and complementing the response capabilities of partner emergency medical teams or non-government organisations (NGOs), by providing disease surveillance and diagnostic testing capabilities.In non-outbreak ‘peace time’, the RRML facilitates operational research, builds capacity through training local scientists, validates locally sourced test results, and strengthens local biosafety and biosecurity measures.
During the creation and expansion of UK-PHRST's RRML, individual components of the lab and the team’s microbiology expertise have been used to support outbreak response, research and capacity strengthening projects across the world. Excitingly, UK-PHRST's Type II RRML is complete and ready to deploy in its entirety, offering its full range of diagnostic capacity. Here are some real-life examples of where components of the RRML and our microbiology team have been deployed.
Outbreak response
St Helena, British Overseas Territory
In May 2026, as part of the wider UK Government response to the hantavirus outbreak, the UK-PHRST deployed a rapid response mobile laboratory (RRML) and three UKHSA staff members to the British Overseas Territory of St Helena.
Photo credit: UK Health Security Agency The team included two microbiologists who provided PCR testing for hantavirus on the island, as well as supporting local testing to exclude other conditions. An infection prevention and control (IPC) expert supported Jamestown General Hospital to prepare and respond to any potential cases, providing IPC assessments and training.
Sudan
In July 2018, Sudan’s Ministry of Health requested UK-PHRST assistance following an upsurge in febrile illnesses of unknown origin in Kassala State. The team deployed both traditional diagnostic methods (RT-PCR and serology) and metagenomic sequencing, which can provide critical insights into the genetic information of the virus.
A total of 142 patients (102 adults, 40 children) with fever (≥37.5°C) and at least three associated symptoms such as headache, arthralgia, vomiting or bleeding were identified for testing at Kassala Teaching Hospital. Blood sample analysis which underwent RNA extraction and RT-PCR testing confirmed Chikungunya virus (CHIKV) in 84.5% of patients, while serological assays for CHIKV and Dengue virus (DENV) differentiated between acute and past infections.
Metagenomic sequencing using the sequence independent single primer amplification (SISPA) method followed by Oxford Nanopore Technologies (ONT) sequencing uncovered the specific strain of CHIKV, its mutations and likely transmission patterns. It also detected DENV co-infections in some patients.
The speed of ONT metagenomic sequencing enabled near-real-time tracking of viral evolution, improving public health decision-making and vector control strategies for preventing future outbreaks. This case demonstrates the value of incorporating metagenomic approaches into routine outbreak investigations,particularly in regions affected by multiple emerging infectious diseases.
Operational research
UK-PHRST's microbiology team is collaborating on several research projects with our partners, including Rapid virus genomics for outbreak investigation (RaViG)- proof of principle in Coastal Kenya. The project, a collaboration between the KEMRI Wellcome Trust Research Programme (KWTRP) in Kilifi, Kenya, the UK-PHRST, the Kenya Ministry of Health and six coastal counties, will assess whether deploying portable whole genome sequencing in real-time during outbreaks is feasible, and if this provides added value to conventional outbreak response approaches.
To build the evidence base, the project team will co-ordinate with local rapid response teams to trial deploying a portable whole genome sequencing system alongside conventional outbreak responses to diseases of suspected or confirmed viral origin. The team will also engage with local and regional stakeholders to evaluateany added value of deploying portable sequencing resource. Microbiology experts from the UK-PHRST are supporting and advising on setting up portable whole genome sequencing in the field during outbreak response, and UK-PHRST epidemiologists are providing scientific evaluation and interpretation.
Capacity Strengthening
The Global Outbreak Alert and Response Network’s (GOARN) strategic group for Diagnostic Surge Capacity (DiSC) created in 2024 is a community of practice of lab specialists and experts, incorporating a network of RRMLs and their parent organisations. The group helps to ensure high-quality diagnostics, seamless cooperation with health systems, and effective emergency response.
Video credits: GOARN Network Before GOARN DiSC was formally established, the RRML network that forms the core of the community set about creating, testing and refining a common set of RRML Minimum Operational Standards. The standards aim to ensure a consistent, high quality and interoperable response between different RRML teams based across the world, who may be jointly deployed to respond to outbreaks.
As a part of the RRML Network, UK-PHRST took part in the first ever Interregional Field Simulation Exercise (IFX): a three-part exercise to review and test the proposed minimum standards across the whole RRML life cycle, from pre-deployment, during outbreak response and end-of-mission phases. The exercise also tested how RRMLs work alongside other WHO health emergency workforce assets, such as Emergency Medical Teams (EMTs), just as in a real outbreak. Read about the highlights, challenges and learnings from the three-part exercise.
UK-PHRST microbiology team members are also part of the GOARN DiSC technical working group creating a WHO certified recognition system for RRMLs, based on the Minimum Operating Standards developed by the RRML Network. UK-PHRST's Director Ed Newman is the current Chair of the GOARN DiSC Coordination Board.
The Rapid Response Mobile Lab: powered by UK-PHRST microbiology expertise
RRMLs cannot function effectively without the experts behind it – microbiologists. The UK-PHRST microbiology team brings diverse expertise in molecular diagnostics, whole genome sequencing, serology, and experience establishing and operating within high-containment laboratories in low- and middle-income countries, often in remote or difficult to access regions.
During outbreaks, their work forms a critical link enabling other specialists like epidemiologists, infection prevention and control teams and social scientists to design and implement targeted interventions. Members of the team have national and international experience with many disease outbreaks including Chikungunya, Crimean-Congo Haemorrhagic Fever, Ebola, mpox, cholera and COVID-19, consistently prioritising peer-to-peer learning, capacity strengthening and international co-operation.

Image credit: WHO Europe UK-PHRST's Rapid Response Mobile Lab - what's in the cases?
The RRML consist of a series of modules - the exact number depending on the scope of the mission - containing several components. Importantly, the availability and number of components is constantly reviewed by the UK-PHRST microbiology team to ensure they can provide the best possible response.
See what's in the cases and find out more about the UK-PHRST's mobile lab
- What does it take to deploy rapidly?
No two outbreaks are the same. Since its inception in 2016, the UK-PHRST operations team can safely testify that there is a need to remain alert, agile, and consistently open to change. Regardless of the mode of deployment, destination or disease, there are always new challenges to navigate.
For example, the suspension of air travel, resulting from border controls during the COVID-19 pandemic, led the team to explore new and innovative ways to offer technical support. Technical expertise was delivered remotely alongside a wide range of partners (including WHO Bangladesh and Africa CDC). This offered opportunities for reservist staff who may not be released for a six-week deployment to volunteer their support.
A full summary of deployments since 2016 can be found below (click to enlarge):
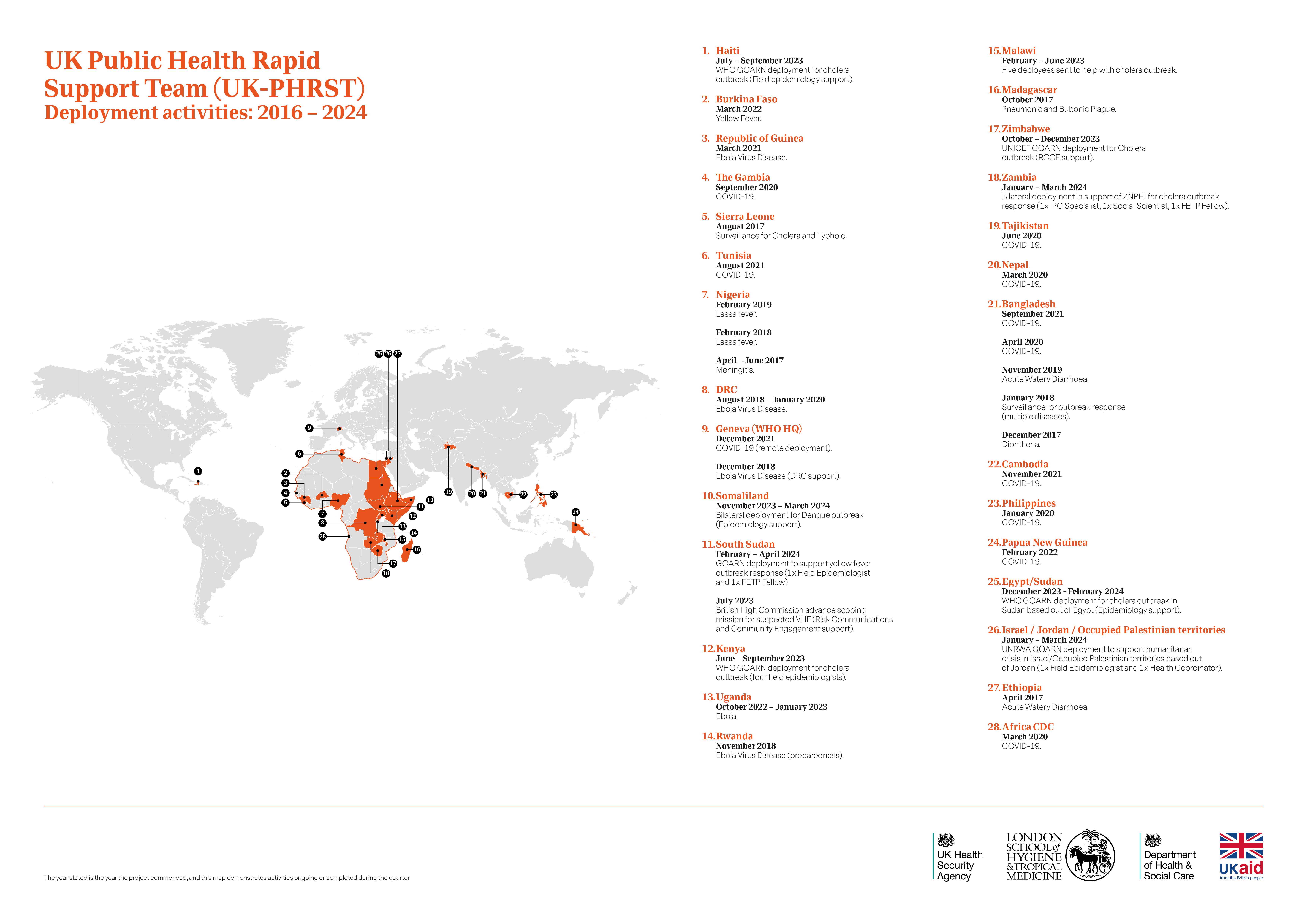
We will summarise the operational requirements to deploy UK-PHRST staff and reflect on what it takes to be operationally ready.
Onboarding staff
Feedback from a wide range of governmental and non-governmental organisations supported the creation of processes to support the onboarding and advanced preparation of deployable staff.
- Medical
It is critical that individuals are medically fit for deployment and have all the necessary routine vaccinations to support their health and wellbeing whilst overseas. A routine schedule of vaccinations alongside a comprehensive medical assessment is required on appointment to the team. Individuals are then issued with an emergency medications kit, first aid kit and trauma kit (and of course, the training on what to do them). - Training
In addition to the necessary technical training, UK-PHRST individuals undertake mandatory UK-PHRST training which aims to prepare them for operating effectively overseas. This includes residential safety and security training, safeguarding training and an immersive 5-day deployment course alongside a package of online learning. - Logistics
Deployed staff are given a comprehensive kit to support their deployment, which includes resources for a wide range of environments (e.g. IT equipment, tents, mosquito nets, water chlorination tablets and ration packs). This kit is systematically reviewed, managed, and maintained by the operations team. external audits of the kit have taken place to ensure rigor and continual improvements are made. - Deployment handbook
This is a guidance document containing all the processes and procedures required of UK-PHRST staff. It incorporates all feedback to date and serves to anticipate any questions relating to finance, medical support, incidents, travel, logistics and more.
Accepting a request to deploy
When the UK-PHRST Director receives a request to deploy, the following steps are taken;
- Criteria – Considerations to deploy include the country, infectious disease agent, location, partners already engaged and threat to further spread (particularly cross border).
- Approval – A Cross-Government protocol (developed in advance with key partners) ensures rapid consideration of any request received by HMG departments. This protocol has been revised several times and represents the key approval mechanism for the team to deploy.
To prepare for deployment:
Once a deployment has been accepted, the team are sent additional information;
- Risk assessment – a travel risk assessment is prepared in advance and includes any known hazards and mitigating actions in relation to the specific deployment, pathogen and country.
- Information pack– includes country and disease specific documentation to aid preparations.
- Pre-deployment briefing – A meeting is set up with the Director, deploying team and key UK-PHRST members to discuss a range of aspects relating to the deployment. This is an opportunity for the individuals to ask any questions and includes, but is not limited to, input from subject matter experts, medical advice, logistics and admin support.
During a deployment
Whilst in the field team members have access to a wide range of 24/7 support from the UK based team. They also benefit from access to a dedicated nurse within the UK Health Security Agency's Occupational Health team.
Reporting of any health and safety incidents or other concerns is done through a systematic process which links in with UKHSA reporting policies.
- Medical
- Making mental health and psychosocial support part of outbreak response
Although mental health affects everyone, whether it’s people trying to maintain their mental wellbeing or those living with a mental health condition, it is often forgotten about in the response to a public health emergency. This is particularly a problem in countries where services are already limited. Before the COVID-19 pandemic, resources allocated to mental health were scarce, with a median of 2% of government expenditure allocated to mental health across the world. During the pandemic, more resources were shifted towards managing COVID-19 infections, making the existing care gap even wider - in a global survey by the World Health Organization (WHO), 93% of 130 countries surveyed reported substantial disruption to their mental health services during the pandemic.
The UK-PHRST has a dedicated Mental Health and Psychosocial Support (MHPSS) team that works particularly across the African and the Eastern Mediterranean regions, on projects ranging from research and capacity strengthening activities to deployments.
The team works to integrate mental health into outbreak response plans and procedures, to improve the mental health and psycho-social wellbeing of people affected, including staff from organisations assisting on the ground – a direct response to the serious impact that these events can have on individuals and communities. During the COVID-19 pandemic in 2020 for instance, global prevalence of depression and anxiety disorders increased by a quarter, with the WHO stating the pandemic “had a severe impact on the mental health and wellbeing of people around the world”.
Strengthening existing MHPSS guidance in outbreaks through research
The team has a diverse research portfolio split into four main phases:
- Phase 1: Identify the needs, resources and current interventions for MHPSS across the African continent
- Phase 2: Work with stakeholders to explore how to better support existing MHPSS frameworks to adapt them into location and outbreak specific response tools
- Phase 3: Test the proposed MHPSS interventions in an outbreak scenario
- Phase 4: Produce a package of MHPSS interventions as a best practice guide which can be applied to specific outbreak situations
The team has already started to see real progress thanks to its research. For instance, members of the UK-PHRST team worked with a consortium of public health institutions in Africa including the Africa Centre for Disease Control (Africa CDC), World Health Organization African Region (WHO AFRO), WHO Regional Office for the Eastern Mediterranean (WHO EMRO) on the Strengthening Public Mental Health in Africa in Response to Covid-19 (SPACE) programme. The programme aimed to help integrate MHPSS into African countries’ emergency responses by exploring the extent to which MHPSS was already included in the national response to the COVID-19 pandemic in African countries. The consortium also examined the barriers and enablers to MHPSS integration in the COVID-19 response. Based on their findings, they recommend five key areas to target for improving mental health integration into the response to public health emergencies. The SPACE programme also acted as a catalyst to the development of working partnerships with regional health bodies and the establishment of an informal network of MHPSS experts across Africa. The research project, alongside other evidence sources, helped inform Africa CDC’s decision to integrate MHPSS into its strategic plan for emergencies.
Building recognition for MHPSS in outbreak response through capacity strengthening
In many countries, current outbreak response infrastructure and national outbreak response plans do not incorporate MHPSS measures. Through its capacity strengthening work, the UK-PHRST MHPSS team actively advocates for MHPSS to be included as part of national outbreak response plans with key health leaders, the strengthening of local co-ordination capabilities and dedication of resources to the area. For example, the team collaborate with Africa CDC to organise workshops throughout African regions to build recognition for the importance of MHPSS in outbreaks, while also taking the opportunity to learn from national MHPSS and emergency response leads to better understand how MHPSS can fit into a local context. In February 2022, the Liberian Ministry of Health, Africa CDC and the UK-PHRST MHPSS team hosted a three day regional workshop bringing together mental health experts from institutions in Africa and worldwide with national mental health leads from Liberia, Sierra Leone, Cameroon and Nigeria. The workshop aimed to build a knowledge and expertise sharing regional network whilst also developing a Theory of Change model for integrating mental health into national emergency preparedness and response plans.

Group attendees of UK-PHRST, Liberian Ministry of Health and Africa CDC Regional MHPSS Workshop. Image credit: Mental Health Innovation Network/Liberian Ministry of Health Finally, the team have also worked directly with organisations like Africa CDC’s African Volunteers Health Corps (AvoHC) to add MHPSS to the list of expertise they provide in public health emergencies in the continent and contributed to WHO Eastern Mediterranean Region’s MHPSS action plan.
Making MHPSS expertise part of outbreak deployments
A lack of global prioritisation for MHPSS during outbreaks, coupled with limited funding and understanding of its benefits, means that MHPSS experts are often not requested during an outbreak response call.
To address this, the UK-PHRST team is actively working to strengthen deployment mechanisms for rapid response, through collaboration AvoHC and IASC/Dutch Surge Support mechanisms. As a part of this collaboration, a group of MHPSS professionals will be trained and prepared to be deployed to ensure that MHPSS is an integral part of the outbreak response.
MHPSS deployments would allow a country to bring in experts to increase its preparedness and response capacity for mental health during an outbreak, allowing other in-country response teams to prioritise the other public health measures that are also required.
Work with the UK-PHRST MHPSS team
If you would like to find out more about the MHPSS team within the UK-PHRST, including how to collaborate or request their help during an outbreak please contact [email protected].

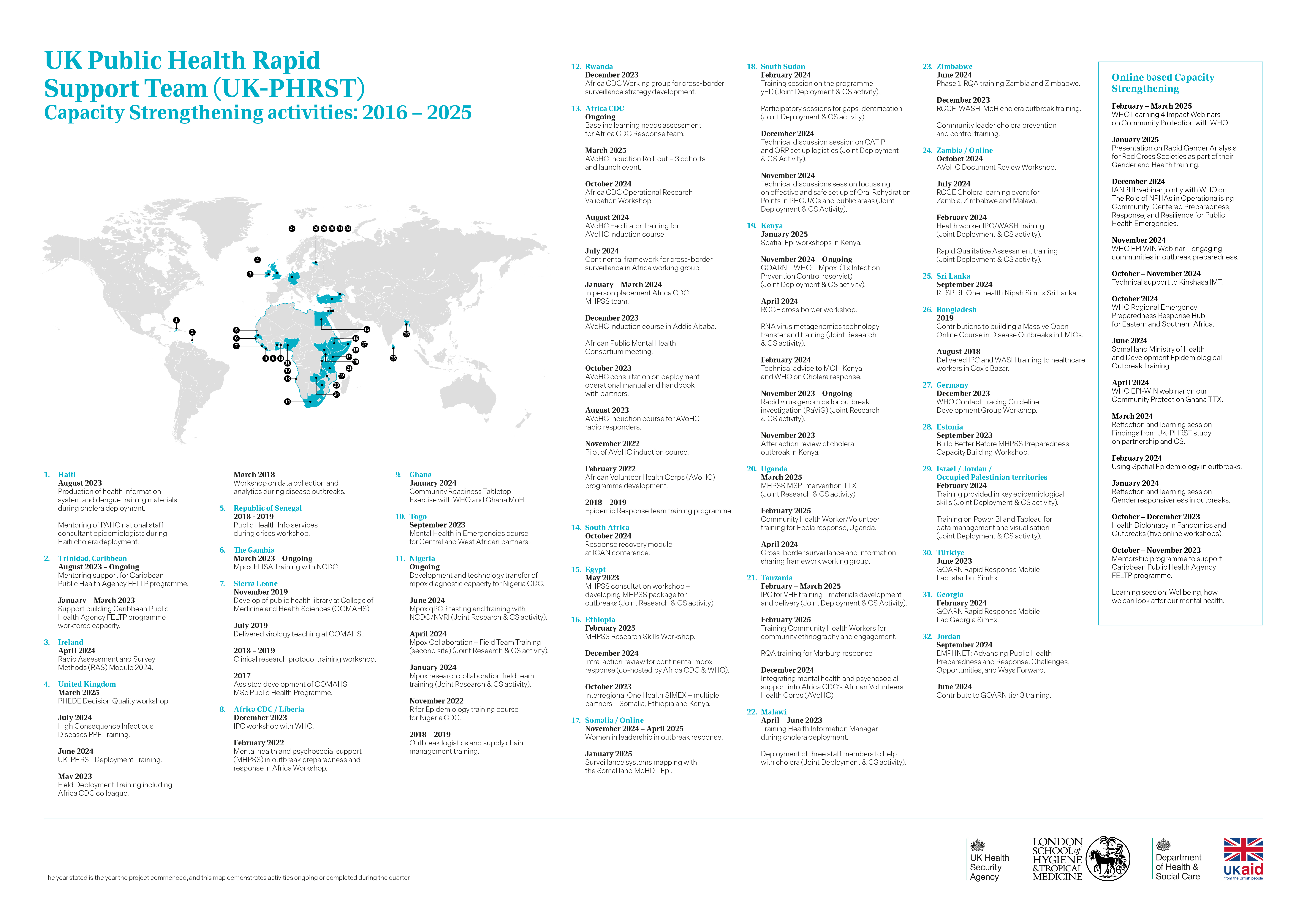{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
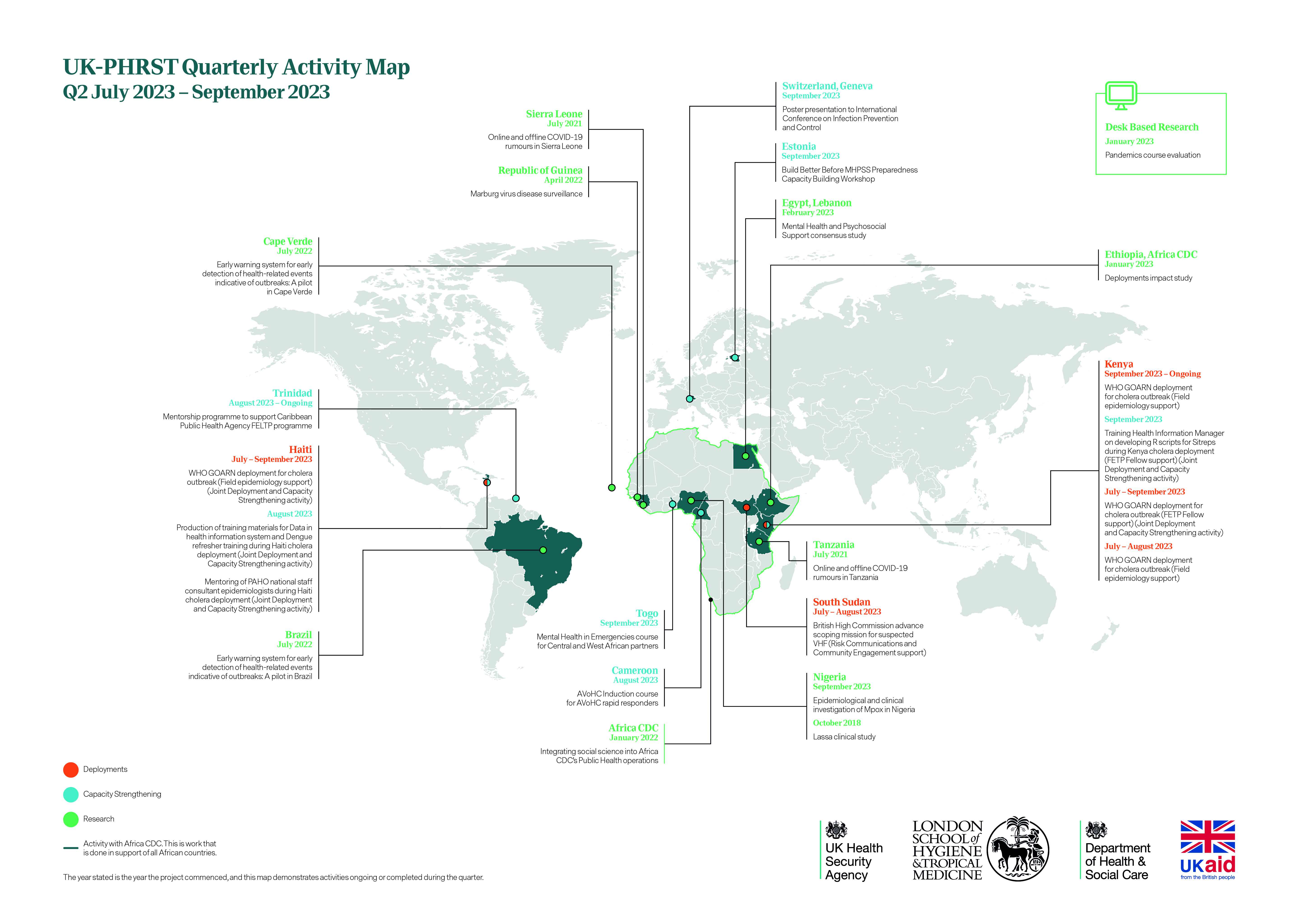{kind=link}
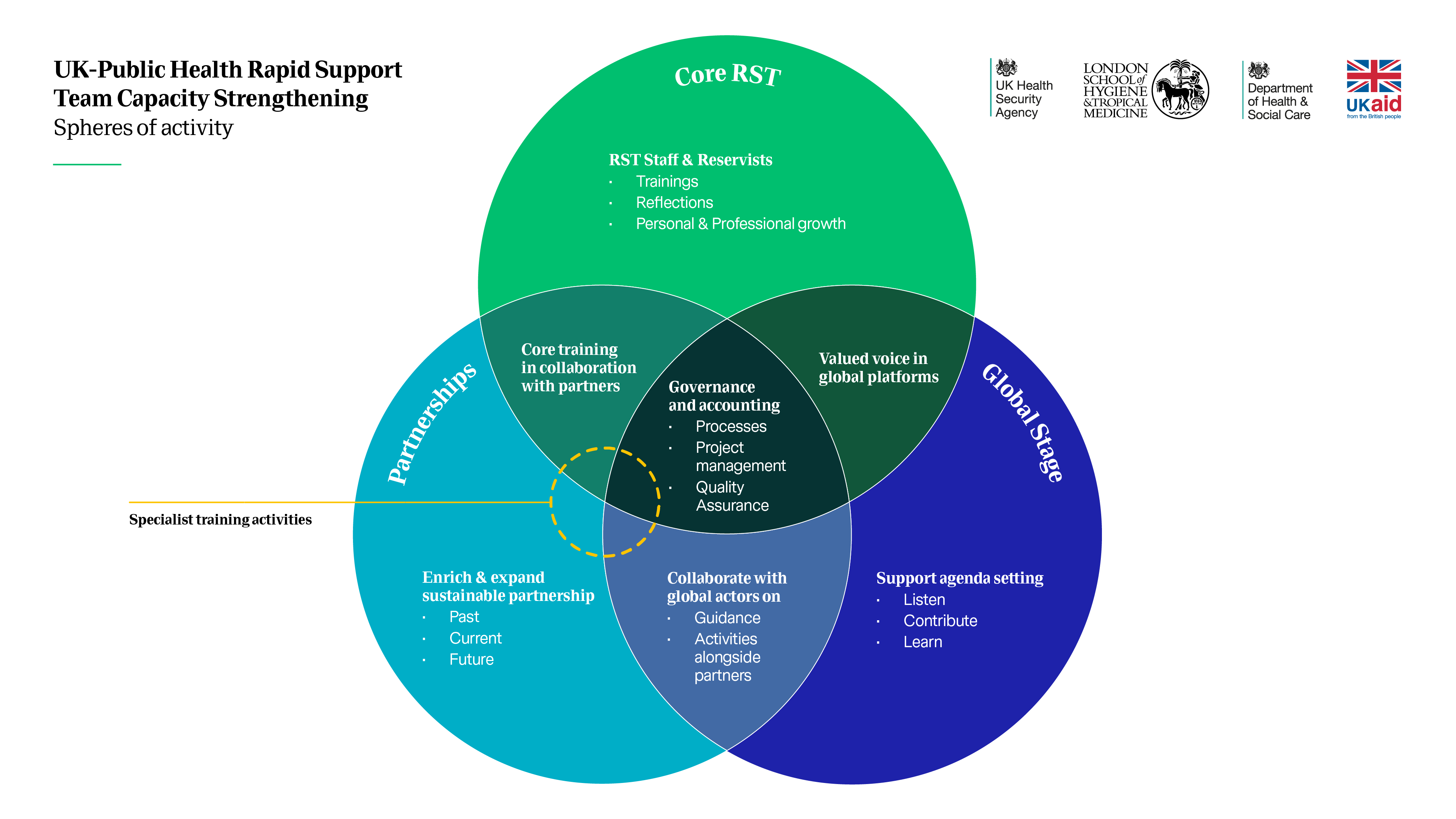{kind=link}
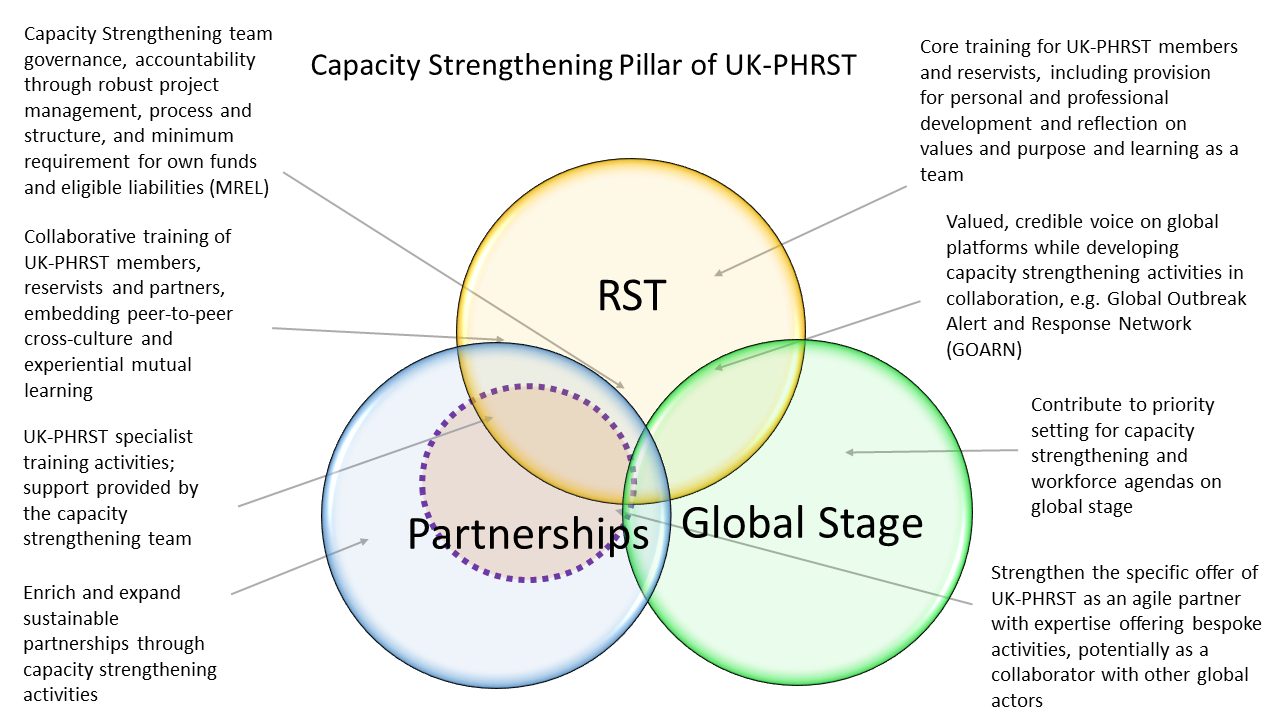{kind=link}
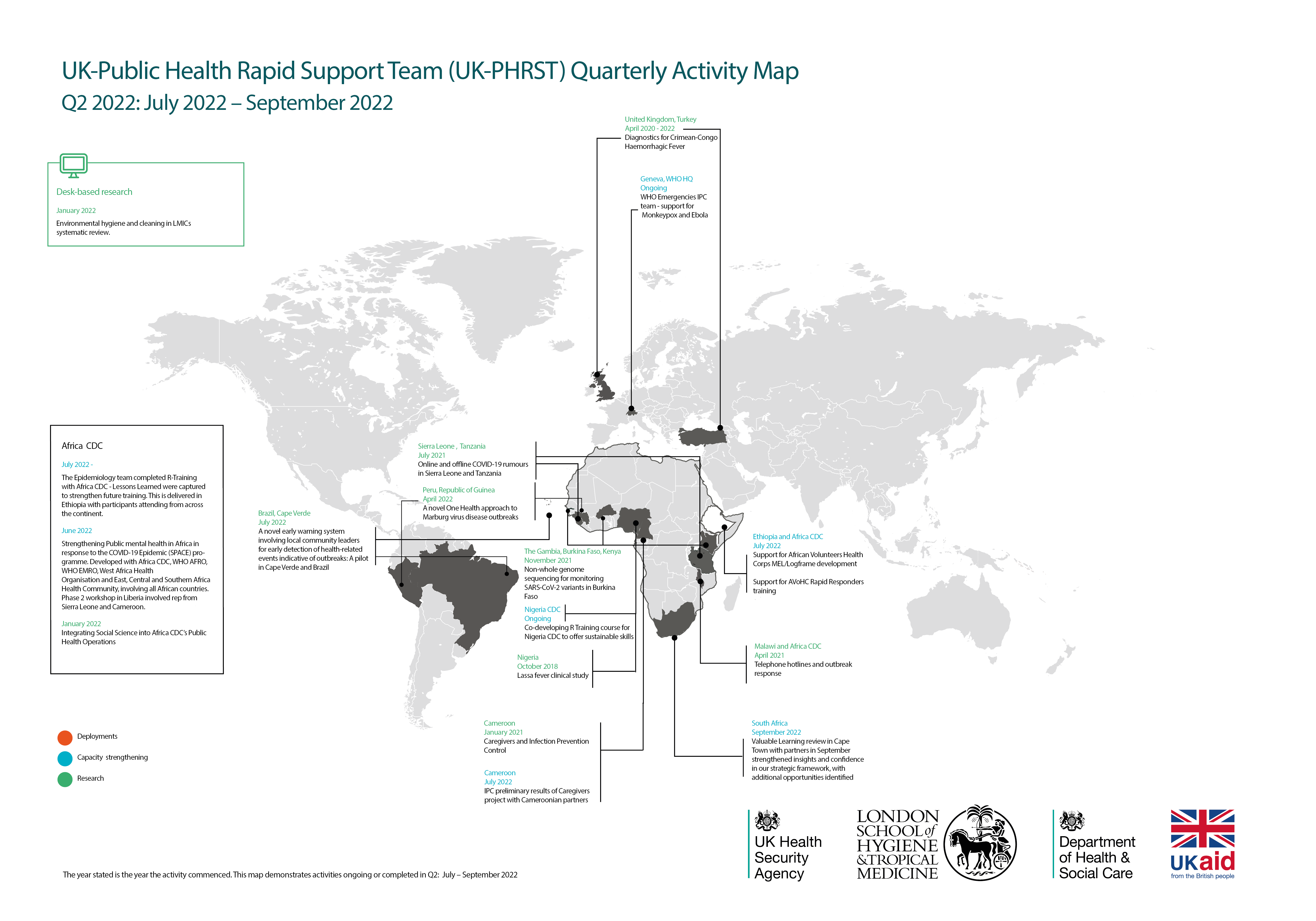{kind=link}
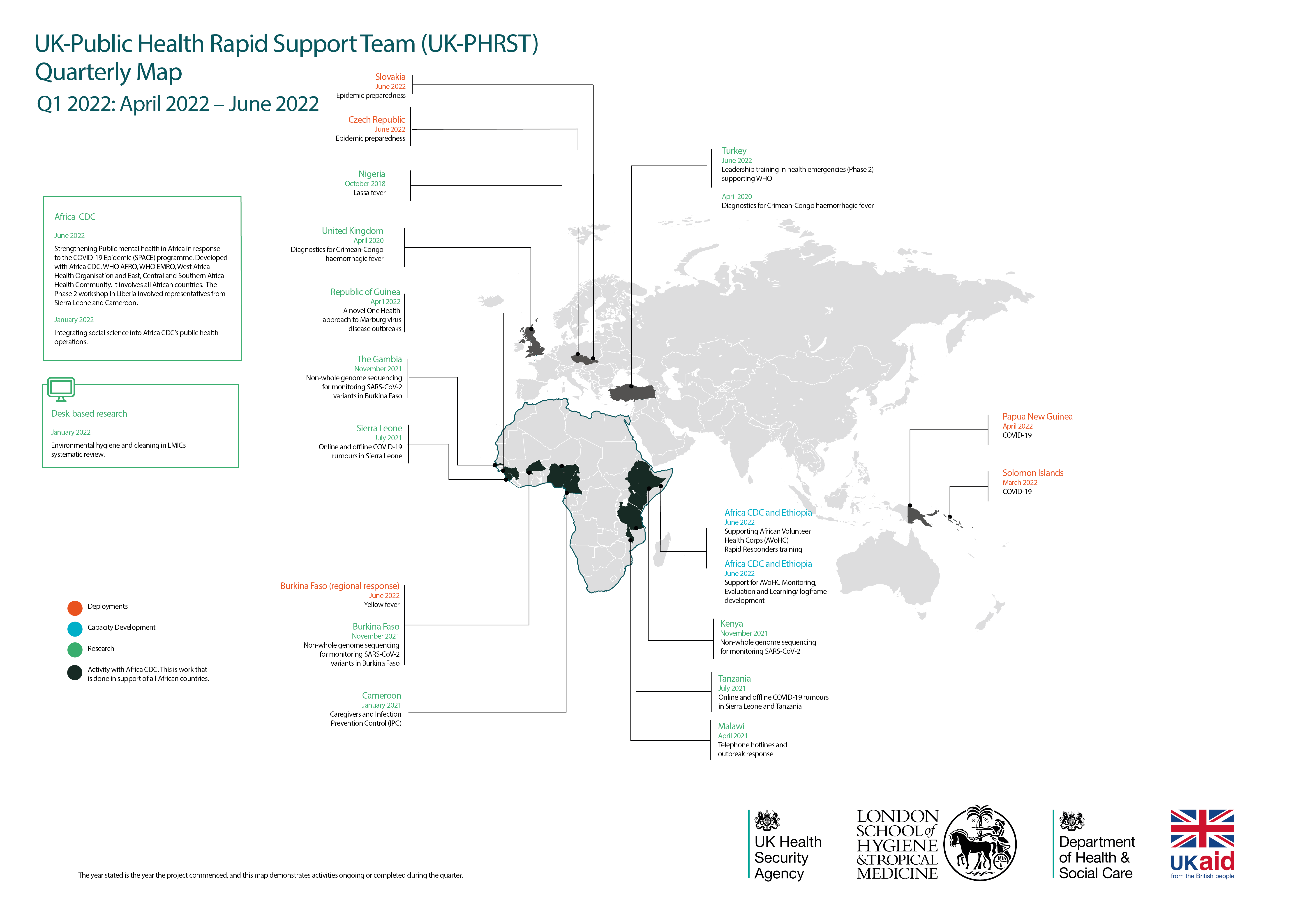{kind=link}