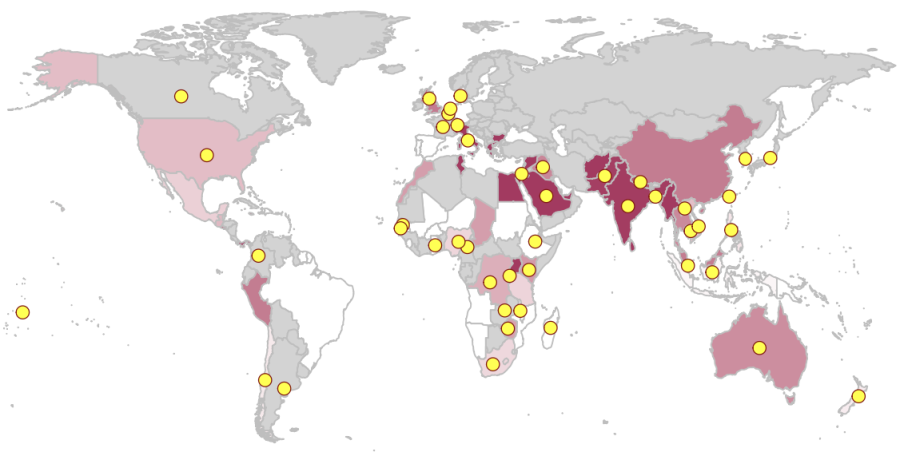
The Global Typhoid Genomics Consortium has published a landmark genomic analysis of the pathogen that causes typhoid fever, providing crucial insights on drug-resistant variants. This collective effort, involving 195 co-authors from 45 countries, provides a comprehensive overview of the genetic diversity and antimicrobial resistance (AMR) patterns of Typhi globally. It marks 22 years since the publication of the first Typhi genome and represents the largest collection of Typhi genome sequences analysed to date, totalling 13,000 samples originating from 110 countries. The Consortium and its first publication are coordinated by LSHTM AMR Centre Co-Director Kat Holt and Centre members Megan Carey and Zoe Dyson, together with colleagues at the University of Cambridge and Oxford University.
The need for genomic surveillance and diagnostic capacity
The new Consortium study highlights wide variation between countries and regions in terms of which variants of the Typhi bacteria are present, and which antimicrobial agents they have evolved resistance to. Most recent genomic studies of typhoid have focused on a specific pathogen lineage or variant, called H58. The H58 variant is concerning because it is frequently drug-resistant, and has spread through Southern Asia and into Eastern Africa. However, by combining data from different countries, the new study shows that other countries have their own local variants that have evolved to be equally drug-resistant. Whether these can spread to neighbouring countries (or have done already) is unknown, and ongoing genomic surveillance is required to monitor this. The study also highlights extensive data gaps, as most countries with endemic typhoid have limited diagnostic capacity to culture the pathogen, let alone sequence it. For many such countries, the available data come from travel-associated cases detected in patients who return home to high-income countries where blood culture and sequencing are routine.
A traffic light system for safe treatment with Ciprofloxacin
Of particular concern is resistance to the drug ciprofloxacin. The World Health Organization (WHO) recommends typhoid patients be treated orally with ciprofloxacin, but only if local resistance rates are low. If resistance is prevalent, treatment should be escalated to oral azithromycin (only suitable for uncomplicated cases) or intravenous ceftriaxone. This makes it critical to understand local resistance rates in different areas. To this end, the Consortium study established a traffic-light system, to reflect whether ciprofloxacin resistance is rare enough to keep using the drug to treat typhoid (<2% resistant – green light), approaching concerning levels (2-10% resistant – amber light), or already too high for the drug to be reliably used (>10% resistant – red light).
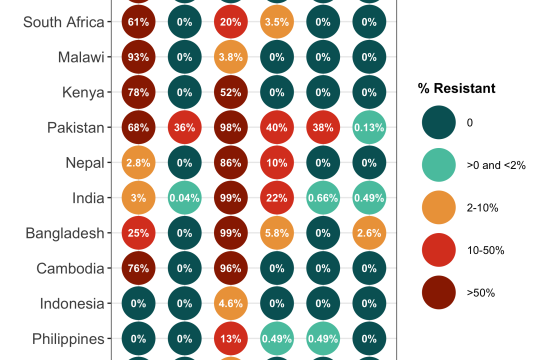
The study confirms that most typhoid infections in South Asian countries are caused by ciprofloxacin non-susceptible Typhi (>85%), and non-susceptibility is also becoming common in some African countries. Importantly, the data show that resistance can emerge in whichever Typhi variants are present in a local setting. So, whilst international transmission does occur, and can contribute to the spread of resistance between countries, all countries are at risk of evolving resistant variants and local monitoring is important wherever typhoid disease occurs. The current lack of widespread surveillance means that ciprofloxacin is likely being used in areas where resistance is already present but undetected, likely leading to prolonged disease episodes with greater chance of onward transmission and severe complications such as intestinal perforations.
Typhoid Conjugate Vaccines
The infectious disease community has watched anxiously since the emergence of an extensively drug-resistant (XDR) typhoid variant in Pakistan in 2016. This variant is resistant to all oral drugs except azithromycin and has caused outbreaks across Pakistan, prompting emergency use of new typhoid conjugate vaccines (TCVs), and more recently, the introduction of TCV into the national immunisation program. The Consortium study confirms that XDR typhoid has not yet become established in other regions. Alarmingly, it did identify variants that are resistant to both ciprofloxacin and ceftriaxone, and azithromycin resistance mutations arising in multiple different bacterial variants across South Asia.
Open access data and tools
The study is quite unique in the world of bacterial genomics research, in its use of an open consortium-driven model. All laboratory groups identified as having published or publicly deposited Typhi sequence data were invited to join the Consortium at its inception in 2021, and membership is open to anyone interested and engaged in typhoid surveillance and sequencing. Members are encouraged to deposit their pathogen sequence data in public archives, and to use a consistent approach to publicly sharing source data (metadata) that is of relevance to downstream public health applications such as estimating local prevalence of bacterial variants and AMR. The consortium uses free and open-access analytical tools and online platforms (including GenoTyphi and Pathogenwatch), for maximal reproducibility and accessibility of their published analyses. Members also support the ongoing development and maintenance of these tools, so that they can continue to be used by public health and research laboratories.
The Global Typhoid Genomics Consortium's primary objective is to encourage sharing of Typhi genomic data and facilitate analysis and visualisation to monitor the emergence and global spread of AMR Typhi. These data can inform decisions concerning the introduction of typhoid conjugate vaccines (TCVs) and other preventative interventions. TCVs can limit the emergence and spread of AMR Typhi, both through the prevention of infections caused by AMR Typhi and a potential reduction in antimicrobial use.
The scale of Consortium’s analysis, which was made possible by a broad network of collaborators, demonstrates the power of open data sharing to enable the extraction of key insights of public health relevance. The group hopes that this serves as a starting point for expanded genomic data sharing and collective analysis, building on the momentum and expanded genomic surveillance capacity developed in response to the SARS-CoV-2 pandemic.
If you enjoyed this article and would like to build a career in global health, we offer a range of MSc programmes covering health and data, infectious and tropical diseases, population health, and public health and policy.
Available on campus or online, including flexible study that works around your work and home life, be part of a global community at the UK's no.1 public health university.