Data and maps are key tools to understand the epidemiology of a disease and to inform the implementation of control measures. Public health interventions at population level have an important impact on the control and elimination of malaria. Malaria maps have been used to plan and monitor malaria control interventions for nearly a century. I was fascinated when I discovered that one of the first maps of malaria distribution was Italian - this year celebrating their 70th year since elimination of the disease. Today, malaria is concentrated in Africa and Asia, and my work looks at data, maps and policies implemented in sub-Saharan Africa (SSA).
Maps of the epidemiology of malaria have changed over time from eco-climatic qualitative maps to more sophisticated maps based on specific indicators, such as incidence or prevalence of malaria. In the last decade, maps based on modelled data have been developed and become available to the National Malaria Control Programmes. The rationale is that, primarily in sub-Saharan Africa, survey or routine data are not always available in time and at the granularity level desired to accurately describe the epidemiological strata; therefore the statistical technique of modelling collates several data (such as prevalence surveys data plus eco-climatic parameters) and models them to develop a picture of the epidemiological situation of the country.
The quality of the maps depends on the quality of the data available. In 2016-2018 I worked with the LINK- data for decision making project in collaboration with KEMRI Wellcome Trust, supporting 14 countries in developing malaria maps based on modelled prevalence data..
As part of the project, we evaluated the perception and use of maps by national malaria stakeholders. Our findings are organised around three topics: use of maps for prioritisation and targeting; use of maps for planning of operational interventions, commodity quantification and advocacy; and factors driving the use by decision-makers.
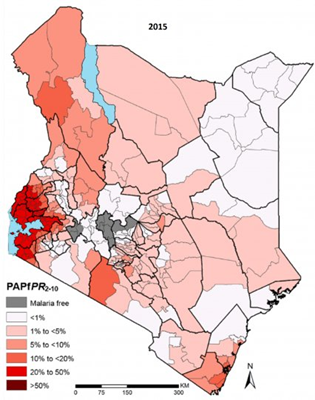
Maps are used for targeting interventions, according to the epidemiological stratification of the country. In Kenya net distribution and chemoprophylaxis for pregnant women are rolled out in specific regions, while in Democratic Republic of Congo (DRC) and Malawi maps are mostly used to target indoor residual spray (IRS) interventions.
Prioritisation of the interventions is not based on maps but on the perceived efficacy of the interventions and on global evidence. “Saving lives” is the first criterion to decide the allocation of the budget which goes firstly to the purchase of malaria medicines (artemisinin combination treatments-ACT) and then to the purchase and distribution of nets.
We observed that epidemiological maps are not used only for planning strategic interventions, but also for planning operational interventions, commodity quantification and internal and external budget advocacy.
The key point of our study was to understand which factors drive the use of risk maps by decision-makers. We understood that the use of maps depends on the perceived needs for an epidemiological map, on the understanding of the way the map was developed (source of data and technique utilised), and on trust and ownership of the data and processes through which they were assembled.
Availability of timely and granularity of geo-located data and heterogeneity of malaria transmission at country level are key in driving the need for developing and use a risk map.
Hopefully these findings will continue supporting National Malaria Control Programmes in developing control tools which would be understood, trusted and used to control and eliminate malaria, as stated by the Malaria Global Technical Strategy 2016-2030.
If you enjoyed this article and would like to build a career in global health, we offer a range of MSc programmes covering health and data, infectious and tropical diseases, population health, and public health and policy.
Available on campus or online, including flexible study that works around your work and home life, be part of a global community at the UK's no.1 public health university.