
1. More support is needed for breast cancer survivors
Millions of women worldwide are living beyond breast cancer, including over 2.7 million in the USA and 500,000 in the United Kingdom. And this number is only set to increase as numbers diagnosed increase and treatments improve. But what is the experience of ‘life after cancer’ for these women?
Our scientists compared 358 breast cancer survivors (roughly 8 years after diagnosis) with 252 women who’d never experienced cancer. They used a questionnaire called the Quality of Life in Adult Cancer Survivors (QLACS), which asks questions about various cancer and non-cancer related aspects of their life in the previous four weeks. To assess mental health, anxiety and depressive symptoms were measured for one week using the Hospital Anxiety and Depression Scale (HADS).
And the findings were profound. Women who’d survived breast cancer had more cognitive problems, sexual dysfunction, fatigue, and anxiety/depression. Issues which were more pronounced if their cancer was advanced at diagnosis or they had been treated with chemotherapy.
These findings paint a clear picture that we need to strengthen interventions to help cancer survivors long after treatment has ended. Currently, eight in ten women with breast cancer in the UK feel they were not warned about the long-term impact of cancer on their mental health, and 41% of women report not having received the professional support needed to cope. To ensure quality of life is maintained for these women, we need to understand what they need to live a full life after cancer and implement new support strategies. Our work is helping to make that a reality.
2. Health-systems can be adapted to improve cancer outcomes. How? With our new model!
It might not be surprising to hear that cancer survival varies greatly worldwide. It might be expected that there are differences between high- and low- income settings. But a mystery presents itself when vastly different survival is seen between two countries with seemingly similar health systems and economies. If it’s not solely income based – then what is causing these differences? And how can policy-makers identify weaknesses in their health systems and change them to improve outcomes? Well, handily, our researchers asked that exact question and came up with a useful model.
So briefly, before getting into specifics, what is a health system? It’s the organization of people, institutions, and resources that deliver health care services to meet the health needs of target populations. In cancer care, for example, this may include a whole host of things: the public’s knowledge around early symptoms, availability of GPs, locations of hospitals and transport links, treatment guidelines, referral processes, waiting times, diagnostic tools, treatment options, staff knowledge, and community care resources (i.e. support groups). Until now, most studies had looked at individual factors that make up these systems, rather than considering the whole system as a living-breathing ecosystem with interlinking parts.
You can see an example of the basic cancer patient care journey below.
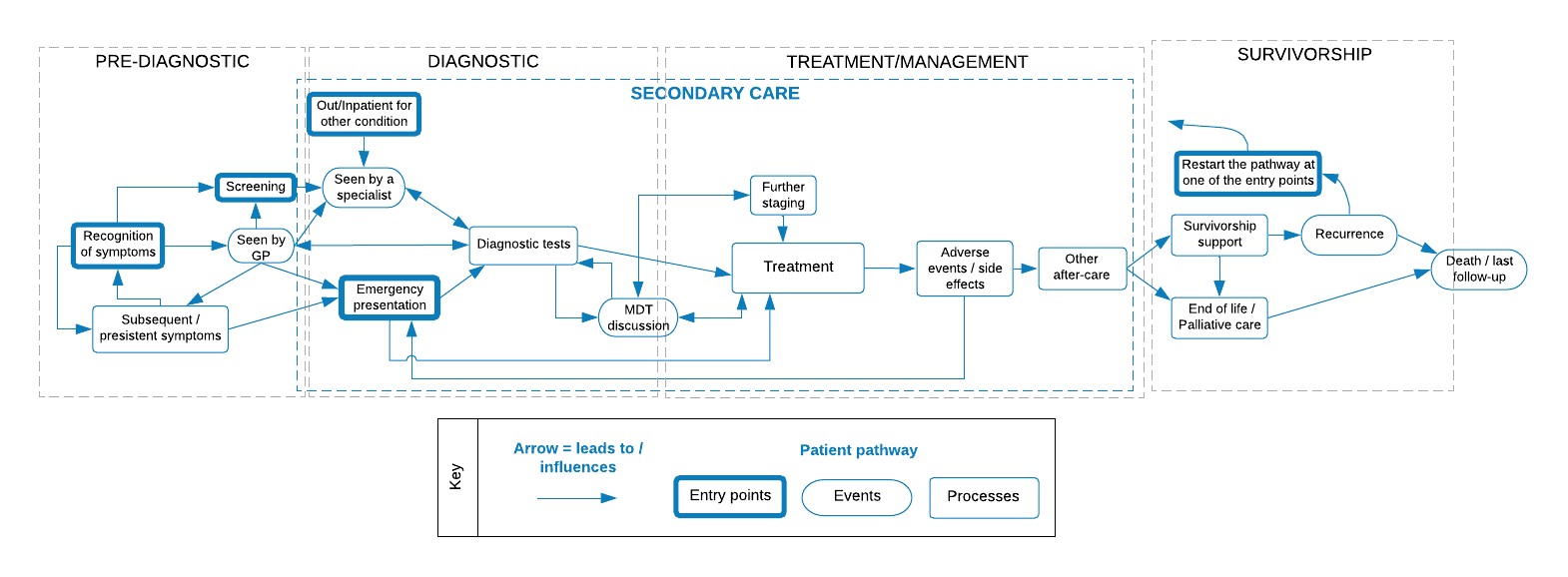
The new ‘logic model’ that we’ve developed incorporates this basic cancer journey, but also all of the health system factors that need to be considered. At each step in the pathway, we’ve added elements and relationships between elements at different levels that are thought to have a role in cancer outcomes. For instance, ‘seen by GP’ seems like a simple step. But actually this relies on patient characteristics (i.e. can they get to/from a GP, can they take time off, are there childcare needs, do they recognise their symptoms?), GP open hours, availability of appointments, GP knowledge, and referral guidelines.
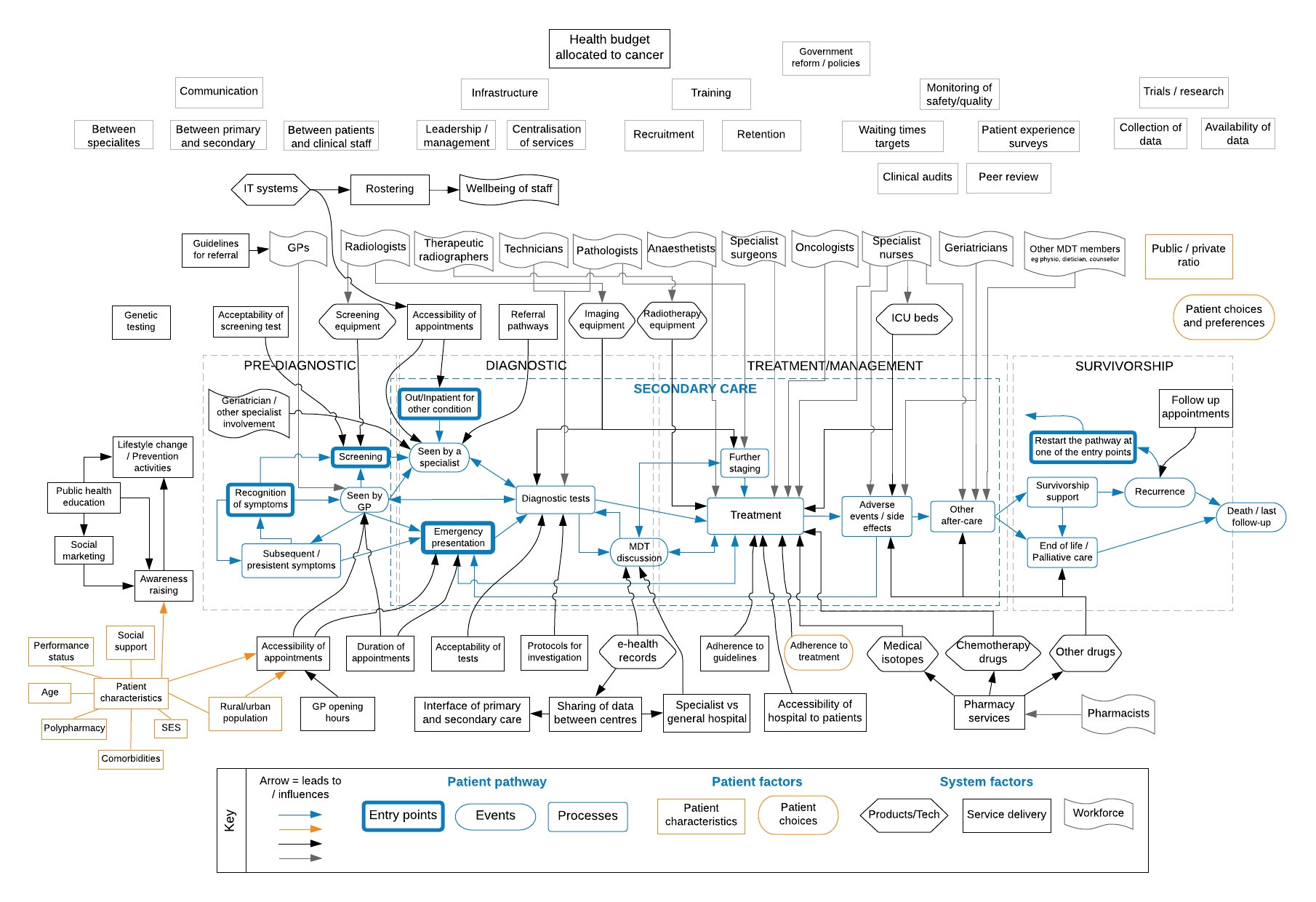
A lot to consider. But this intricately interconnected framework is a vital tool for policymakers, practitioners and researchers seeking to improve cancer outcomes. It enables them to take a critical look at each stage of the patient journey, consider the complex interactions between factors at different levels, and identify areas for improvement or optimisation. Even better – the model can be adapted to an individual cancer site or used to look at a higher level for the whole cancer care system. Through implementation of this approach the hope is to close the gap in cancer survival so that all patients, no matter where they are in the world, have access to the best quality care and chance of survival.
3. People with Atopic Eczema may be at increased risk of Lymphoma – but not any other cancer types
Competing theories have been flying around the scientific literature as to the link between atopic eczema and cancer. To briefly cover the competing rationales – people with atopic eczema have an enthusiastic immune system. But increased immunity can be both a good or bad thing when it comes to cancer. On the one hand – more patrolling immune cells means more chance of spotting a ‘rogue’ cell and eliminating it before it can become a tumour. But immune cells also tend to produce a lot of inflammation, and cancer cells LOVE a nice inflamed environment – it’s their version of a nightclub with plenty of food and drink flowing to lure in and convert other cells to their rebellion.
But if we are developing new ‘biological’ treatments for eczema, it’s important we know if either (or neither) of the above is happening as a baseline. That way, if the new treatments represent a risk, we’ll be able to directly compare. So our scientists decided to settle it once and for all – using some pretty hefty datasets!
From England, they identified a cohort of more than 450,000 people with, and more than 2.2 million patients without, atopic eczema. And from Denmark almost 45,000 and just under 450,000 people with and without atopic eczema respectively.
They then compared overall cancer risk and risk of specific cancers in these people with and without atopic eczema. On average, they followed the English participants up for four and a half years and the Danish cohort for just over 14 years.
In both countries, little evidence was found of any association between atopic eczema and overall cancer. But, there was evidence of larger increases in lymphoma risk in those with eczema. In England, the risk of non-Hodgkin and Hodgkin lymphoma was 20% and 48% higher respectively in people with atopic eczema compared to people without. And the risk increased with severity of eczema.
As with most research, as one answer is provided, many more questions emerge. In this case, it’s important to understand why there’s an increased lymphoma risk among people with atopic eczema. Is it that eczema is an early warning sign for lymphoma? Is it linked to the Epstein-Barr virus? And what are the therapeutic implications? Perhaps by World Cancer Day 2022, we’ll have some more answers.
If you enjoyed this article and would like to build a career in global health, we offer a range of MSc programmes covering health and data, infectious and tropical diseases, population health, and public health and policy.
Available on campus or online, including flexible study that works around your work and home life, be part of a global community at the UK's no.1 public health university.