
We conduct research to understand the implications and effects of community involvement and dialogue in promoting health, planning health services, and quality improvement of existing services.
Our work spans six key research themes
- Health experiences and practices
- Community participation and co-production
- Transitions to adulthood
- Evaluation and methodology
- Ethics and epistemology
- Digital lives
Find out more about our work on community participation, patient engagement, and dialogues for health - including plain-English summaries
Meet the DEPTH team at London School of Hygiene & Tropical Medicine.
We conduct research to understand the implications and effects of community involvement and dialogue in promoting health, planning health services, and quality improvement of existing services.
- Health experiences and practices
-
Using interviews and other innovative ways to elicit voices and experiences, we explore how social lives and health practices are intertwined. Much of our work involves dialogues about sexual and reproductive health and practice in diverse communities around the world. Examples include the sixteen18 project which explored young people’s sexual practices in the UK, and our Ghana project where we interviewed women about their fertility practices. Our work shows how introducing and promoting more honest and critical dialogues about sexual and reproductive health improves understanding of complex dynamics in relationships and hidden practices.
When it comes to health experiences, voice is key. Our recent project 'This Sickle Cell Life', a sociological study of young people's experiences of paediatric to adult healthcare transitions, highlighted the importance of listening to the voices of young people with sickle cell. In this project and across our work, we examine the implications of dialogue for understanding experiences and developing more inclusive forms of knowledge. We also explore which voices are heard in conversations about health and which are left out.
- Community participation and co-production
-
Our work on community participation and citizenship has involved long term ethnographic explorations of public and patient involvement and engagement in research and quality improvement in the UK National Health Service. This research has helped us build theory around community participation, engagement, and empowerment, their effects, and the implications for citizenship in health. This work also addresses practical aspects of how to make participation successful such as how to create effective and inclusive spaces for participation, and how to orientate organisational culture so it helps rather than hinders participation.
Our international activities include work with the WHO (World Health Organisation) on guidelines on community participation to promote maternal and newborn health, as well as informing the ‘community engagement’ action area of the Global Strategy for Women’s, Children’s and Adolescents’ Health.
The COVID-19 pandemic highlights the crucial importance of dialogue, evidence, and participation for health. Dialogue and co-production are essential for effective pandemic response. Global health guidelines already emphasise the importance of community participation, but in a pandemic, it is more important than ever to involve communities in planning and response. Marginalised communities and individuals are disproportionately harmed by COVID-19 and those communities are best-placed to know what is most needed to help them. Co-production – collaborative work between researchers, clinicians, patients and the public – can improve health, and help reduce inequalities by addressing diverse needs and helping ensure that actions do not cause harm. Co-produced healthcare responses to COVID-19 are more likely to address specific needs, identify gaps in policy, and find solutions by working together.
- Transitions to adulthood
-
Our work has examined young people’s transitions to adulthood, ways that sexuality, sexual practice and contraception are bound up in life experiences and identity, and health and wellbeing of adolescents and young people.
In This Sickle Cell Life, we took a sociological approach to look beyond the clinical realm into other areas relevant to transitions to adulthood such as education and social relationships. Working in collaboration with patient representatives, social scientists, clinicians and quality improvement experts, the project facilitated dialogue about how transitions into adult healthcare can be improved, including how to improve health services for people with sickle cell.
- Evaluation and methodology
-
Developing evaluation methodology, particularly for complex social interventions, is a core interest for the team. Our recent work has included developing ways to evaluate a partner violence prevention intervention for young people that was part of a comprehensive sexuality education programme, how to investigate 'context' in evaluations, and ways to evaluate SRHR interventions for marginalised populations in complex and challenging environments in our lead research role for the ACCESS consortium.
- Ethics and epistemology
-
Accurate science communication is crucial if people are to make informed decisions about their health. We work with the World Health Organization to ensure that global guidelines are based on the best interpretation of the scientific evidence. We also work with other groups such as COMPare in Oxford to investigate potentially unethical practices in trial reporting. We have debunked false claims about abortion and also revealed how inappropriately optimistic effectiveness claims about a version of the rhythm method (the Standard Days Method) are being used to heavily promote it in low-income settings.
Conducting and communicating our research in an ethical way is key to promoting valuable dialogue with a range of people. By acknowledging the gaps in the way that researchers listen to participants, we can think of ways to improve on taking our lead from the participant. We want to amplify the voices that are less heard.
- Digital lives
-
We are increasingly investigating digital life as a key mediator of dialogue, personhood and community. We are particularly interested in how dialogues are promoted and restrained in increasingly digital lives, and the interrelationships between digital lives and health.
Our work includes advising government and providing commentary and analysis on effects of pornography on young people, and theoretical explorations of the use of mobile phone locative media apps such as Grindr and Tinder for sexual partner seeking.
We have also examined public views and experiences of using electronic health records for research.

The COVID-19 pandemic highlights the crucial importance of dialogue, evidence, and participation for health. DEPTH is committed to inclusive, participatory action in the COVID-19 response.
Dialogue and co-production are essential for effective pandemic response
Global health guidelines already emphasise the importance of community participation, but in a pandemic, it is more important than ever to involve communities in planning and response. Marginalised communities and individuals are disproportionately harmed by COVID-19 and those communities are best-placed to know what is most needed to help them. Co-production – collaborative work between researchers, clinicians, patients and the public – can improve health, and help reduce inequalities by addressing diverse needs and helping ensure that actions do not cause harm. Co-produced healthcare responses to COVID-19 are more likely to address specific needs, identify gaps in policy, and find solutions by working together.
Pandemic responses have largely involved governments telling communities what to do, seemingly with little community input. We are concerned that the few existing spaces for community participation in the UK such as in the NHS are being shut down and overall, citizen participation is noticeable by its absence.
Communities clearly want to help: in the UK half a million people volunteered to help the NHS pandemic response, and highly localised mutual aid groups are springing up all over the world in which citizens help one another with simple tasks and check on wellbeing during lockdowns. The most vulnerable and ignored groups can help identify solutions: they know what knowledge and rumours are circulating; they can provide insight into stigma and structural barriers; and they are well placed to work with others from their communities to devise collective responses.
Working with communities means collaborating to create tailored ways to meet the full needs of our diverse populations. Community-led responses are also more likely to be acceptable, feasible, and sustainable.
Marston, Renedo, Miles. 'In a pandemic community participation is crucial.' Read the full article we published in The Lancet, May 2020.
Co-production in the COVID-19 pandemic is extremely challenging, but our past work shows how important it is to involve communities. Find out more about our research on community participation and patient and public involvement in healthcare:
- Addressing sexual and reproductive health and rights in crisis
In times of crisis, sexual and reproductive health and rights are often not prioritised. With all areas of the health system strained by the emergency response to COVID-19, there is a risk that resources for sexual and reproductive health services may be reduced or diverted, particularly in low-resource settings, compromising or harming sexual and reproductive health and rights – particularly for the most marginalised.
As part of the ACCESS consortium, DEPTH proposes to research how best to work with communities to co-produce pandemic response to SRHR needs for the most marginalised people living in complex and challenging environments including humanitarian settings. Read more about our proposed work.
- Ensuring the pandemic response includes the most marginalised
DEPTH co-produced research into the impacts of sickle cell disease. This Sickle Cell Life, has already demonstrated how chronic health conditions shape young people’s lives, and, crucially, the negative consequences of failing to involve patients as experts in their own condition. Our collaborative research with patient and carer experts identified key challenges which are likely to be exacerbated with COVID-19, including failure of non-specialist hospital staff to understand or meet the specific needs of people with sickle cell, leading to poor care. Failing to involve patients in healthcare responses to the pandemic risks amplifying existing disadvantages and inequities for the most vulnerable. Read more about This Sickle Cell Life.
- Build back better, more sustainable, more inclusive healthcare
Our work has shown how important it is to involve communities to improve health worldwide. We must include communities throughout the response, and when we rebuild, draw on those same engagement networks and community groups to ensure that damaged health systems are more efficient, more inclusive, and more robust to shocks and crises.
DEPTH work has been incorporated into the Community Engagement action area of the Global Strategy for Women’s,Children’s and Adolescents’ Health, and DEPTH researchers participate in the WHO-convened Community of Practice on Social Accountability. We research community participation in healthcare, including in times of crisis, to understand how to co-create an effective, sustainable response.
- Developing community involvement and co-production even in lockdown
DEPTH will work with ACCESS consortium partners to investigate how community involvement is maintained in crisis and whether the most marginalised are being included. We will investigate ways to strengthen existing networks and set up new ones in the most complex and challenging environments to ensure nobody is left behind.
- Learn what works, when, how, and for whom
We will advance global understanding of how to improve sexual and reproductive health in crises, attending to the social context of interventions, and intended and unintended impacts on equity and rights. We will explore co-production, participation and impact of complex interventions in dynamic contexts, drawing both on the methodological expertise within DEPTH and that of our colleagues in the Centre for Evaluation, and on our work on the nature of co-production, patient engagement, and community participation.

Routes: new ways to talk about covid for better health. Focus on Gypsy Roma and Traveller communities, and migrant workers in precarious jobs
Overview
Gypsy, Roma and Traveller communities and migrant workers often experience worse health than the general population, with existing inequalities exacerbated further by the Covid-19 pandemic. Understanding health experiences within these communities and co-designing solutions is vital to improve health equity and health services.
The project involves participatory research with Gypsy, Roma and Traveller communities, and with migrant workers in precarious jobs, using our ‘DEPTH’ approach, to identify and address barriers to good health. We work with policymakers, healthcare staff, and communities to generate rigorous evidence and to co-produce research and solutions that are tailored, meaningful, feasible and effective.
Our approach involves community members as co-researchers to ensure that we ask the right questions, contextualise the responses properly, and find solutions together. We are exploring real life experiences relevant to Covid-19 risk, prevention and response, and co-producing solutions via dialogues about the findings. By co-producing the research, we will understand specifics of health experiences and needs, and how best to address them. While we are focusing on Covid-19 prevention, we anticipate that our findings will also be transferable to other areas of health.
Outcomes
By using our DEPTH approach, particularly as it relates to community participation in Covid-19 health responses we will generate rigorous evidence, and co-produce recommendations that are evidence-based, address real community concerns, and are acceptable and feasible.
We aim to promote dialogue and generate knowledge, with Gypsy, Roma, Traveller, and migrant worker communities, to understand:
- experiences of the Covid-19 pandemic;
- experiences and views of public health responses to Covid-19;
- when and why people do or do not engage with different elements of Covid-19 prevention, taking account of broader issues with engagement with health services;
- how people's living and working conditions affect their ability to protect themselves from Covid-19 and to engage with health initiatives, focusing on test and trace;
- Understand the broader social context affecting people’s lives and how this affects health and use of health services.
Using evidence from the project we will then engage in dialogues with communities and other key stakeholders to co-produce recommendations relevant to the public health response to Covid-19.
Outputs
Project outputs included regular ‘three key findings’ policy briefs delivered to the policy teams at regular intervals during the project. There are five publications, all free to download:
- Kühlbrandt, Charlotte; McGowan, Catherine R; Stuart, Rachel; Grenfell, Pippa; Miles, Sam; Renedo, Alicia; Marston, Cicely; (2023) COVID-19 vaccination decisions among Gypsy, Roma, and Traveller communities: A qualitative study moving beyond "vaccine hesitancy". Vaccine, 41 (26). pp. 3891-3897. ISSN 0264-410X DOI: https://doi.org/10.1016/j.vaccine.2023.04.080
- Miles, Sam; Renedo, Alicia; Kühlbrandt, Charlotte; McGowan, Catherine; Stuart, Rachel; Grenfell, Pippa; Marston, Cicely; (2023) Health risks at work mean risks at home: Spatial aspects of COVID-19 among migrant workers in precarious jobs in England. Sociology of health & illness. pp. 1-18. ISSN 0141-9889 DOI: https://doi.org/10.1111/1467-9566.13711
- Renedo, Alicia; Stuart, Rachel; Kühlbrandt, Charlotte; Grenfell, Pippa; McGowan, Catherine R; Miles, Sam; Farrow, Serena; Marston, Cicely; (2023) Community-led responses to COVID-19 within Gypsy and Traveller communities in England: A participatory qualitative research study. SSM - Qualitative Research in Health, 3. 100280-. ISSN 2667-3215 DOI: https://doi.org/10.1016/j.ssmqr.2023.100280
- Stuart, Rachel; Grenfell, Pippa; Renedo, Alicia; McGowan Catherine R; Kühlbrandt, Charlotte; Miles, Sam; Marston, Cicely. Necropolitics and Necroresistance: Qualitative Research with Gypsy, Traveller and Roma Communities During the COVID-19 Pandemic. British Society of Criminology Online Journal Vol 22 pp.24-38
- Marston, Cicely; McGowan, Catherine; Stuart, Rachel; Kuhlbrandt, Charlotte; Miles, Sam; Grenfell, Pippa; Dix, Laura; Renedo, Alicia; (2022) Routes: new ways to talk about COVID-19 for better health (final report) A focus on Gypsy, Roma and Traveller communities, and migrant workers in precarious jobs. Project Report. DEPTH Project, London. https://researchonline.lshtm.ac.uk/id/eprint/4669580
This project was funded by NHIR Public Health Policy Research Unit. Read more about the project, and other NIHR Public Health Public Health Policy Research Unit projects.
ACCESS: Improving sexual and reproductive health and rights in complex and challenging environments
In 2019 LSHTM researchers began an ambitious piece of work funded by UK Aid: the ACCESS consortium, led by the International Planned Parenthood Federation, aimed to improve sexual and reproductive health and rights (SRHR) in complex and challenging environments including humanitarian settings in Nepal, Uganda, Mozambique and Lebanon.
Contraception and safe abortion care services, HIV/STI prevention, treatment and care, and comprehensive sexuality education are often poor or unavailable to marginalised groups in many parts of the world. Multiple complex and interconnected barriers impede universal access to good SRHR. Access to rights-based services, such as contraception and comprehensive sexuality education, is often compromised or denied, and barriers to achieving SRHR, including sexual and gender-based violence (SGBV), may disproportionately affect marginalised groups.
Funded by UK Aid (initially via the UK Department for International Development, later the Foreign, Commonwealth & Development Office) the Approaches in Complex and Challenging Environments for Sustainable SRHR (ACCESS) Consortium (2019-21) created innovative solutions to ensure that marginalised people including young people, disabled people and refugees are not left behind.
The ACCESS consortium was led by the International Planned Parenthood Federation (IPPF) and was selected within the UK Aid Connect programme. LSHTM partnered with IPPF, Frontline AIDS, the Women’s Refugee Commission, the Open University and Internews, bringing a wide range of expertise to generate sustainable, scalable, rights-based approaches to deliver comprehensive SRHR to all. The research was led by the Dialogue, Evidence, Participation & Translation for Health (DEPTH) research group in collaboration with academic staff from across the institution, under the leadership of Professor Cicely Marston, principal investigator for LSHTM, Director of the DEPTH research group, and research director for the consortium. The co-creation phase (April 2019-March 2020) was completed, but the main, implementation phase of the consortium work was delayed by the pandemic and began in October 2020.
LSHTM’s role within the consortium was to lead on research, creating a strong evidence-base for what works to improve sexual and reproductive health and rights (SRHR) for the most marginalised groups living in complex and challenging environments, including humanitarian settings.
We planned to do this through three interconnected workstreams:
- Formative research into lives, needs, contexts and services: we planned to conduct research to understand the lives and needs of marginalised people and how we might improve their sexual and reproductive health and rights (SRHR). This research would have informed interventions and advance knowledge.
- Evaluations of ACCESS consortium programme components: we were planning to evaluate the extent to which ACCESS mini-projects improve Sexual Reproductive Health and Rights (SRHR).
- An evaluation of the ACCESS participatory approach as a whole (‘Practising, understanding and measuring participation’): we aimed to try to understand how participation and co-production work in practice to improve SRHR (including understanding and measuring participation and its effects across programme activities) and generate transferable insights to improve implementation of inclusive and successful participatory practice in other settings.
Policy barriers, lack of understanding about the needs and preferences of marginalised groups, and ineffective interventions all contribute to inadequate sexual and reproductive health and rights. LSHTM, and the ACCESS consortium, took a participatory approach, using the latest methodologies to work with partners and beneficiaries with the aim of developing and testing the effectiveness of a range of interventions, generating new evidence and making recommendations that will improve people’s health and wellbeing
The ACCESS consortium was axed by the UK government without warning in April 2021, six months after the implementation phase began, as part of the UK aid budget cuts. Nevertheless, we produced some useful outputs.
‘Global Goods’
We have developed ‘Global Goods’ from this project, listed below:
- Publication on Making authorship guidelines that promote equity in co-produced academic collaborations
- Article Methods to measure effects of social accountability interventions in reproductive, maternal, newborn, child, and adolescent health programs: systematic review and critique in the Journal of Health, Population and Nutrition
- BMJ Opinion blog on Covid-19 in humanitarian settings: addressing ethics to reduce moral distress
- Article Preparing humanitarians to address ethical problems’ in Conflict and Health
- Article on COVID-19 testing acceptability and uptake amongst the Rohingya and host community in Camp 21, Teknaf, Bangladesh in Conflict and Health
- Article on making a graphic elicitation technique to represent patient rights in Conflict and Health
- Our commentary with WHO Community of Practice, Unpacking power dynamics in research and evaluation on social accountability for sexual and reproductive health and rights.
- Our protocol for Sexual and reproductive health service considerations for people of diverse sexual orientation, gender identity and expression, and sex characteristics (SOGIESC): a systematic review
- Our Lancet commentary publication Community participation is crucial in a pandemic
- Our blog post Who writes what? Responsible authorship recognition in co-produced research at our LSHTM DEPTH website (September 2021)
Check out previous DEPTH blog posts here.
Our latest blog is by our former DEPTH Project Manager Laura Dix, who reflects on 18 months working with us in collaborative research at LSHTM. Laura offers a brilliant perspective that we don’t always gain ourselves from the ‘inside’ - here are her top 5 reflections on collaboration…

Co-production. Co-creation. Expert-led. Service User Involvement. Patient Public Involvement.
Whatever you want to call it, in recent years collaboration and partnership with communities has become a more visible and debated practice in many different sectors, from global NGOs to local government to academia.
This shift is an important one. Who wouldn’t argue that the people most affected by an issue should have a say not only on how it is defined, but what solutions are put in place? However, the language of “involvement” has come to cover multiple different methods of engagement, ranging from truly equal partnerships to just a label slapped on a project to make it sound good.
I came from the charity sector in October 2020 to join the DEPTH Team at LSHTM, who are specialists in involving communities in research to promote health and equity. I was fascinated to find out how the experts ‘do’ involvement, and what differences there might be in the jump from an NGO to academia. So after 18 months as a fly on the wall in my excellent team, what have I learned about co-production? Here are my top 5 reflections…
1. It can be helpful to broaden your definition of community
We often talk about community involvement in terms of how we engage patients, service users or clients, but it can also be helpful to expand this definition of “community” and include within it others that are participating in the project - for example our colleagues, external stakeholders, consultants and co-researchers.
Once we see a project as having multiple communities of interest, it might be helpful to also use models of co-production to understand and take into account different levels of interest, involvement and input that various people want, or are able, to input on a project. This has the benefit of helping to build relationships and knowing who to engage with, and at what level that engagement happens. For example, many user involvement approaches show it as a sliding scale or as a ladder, such as this one from Passio:
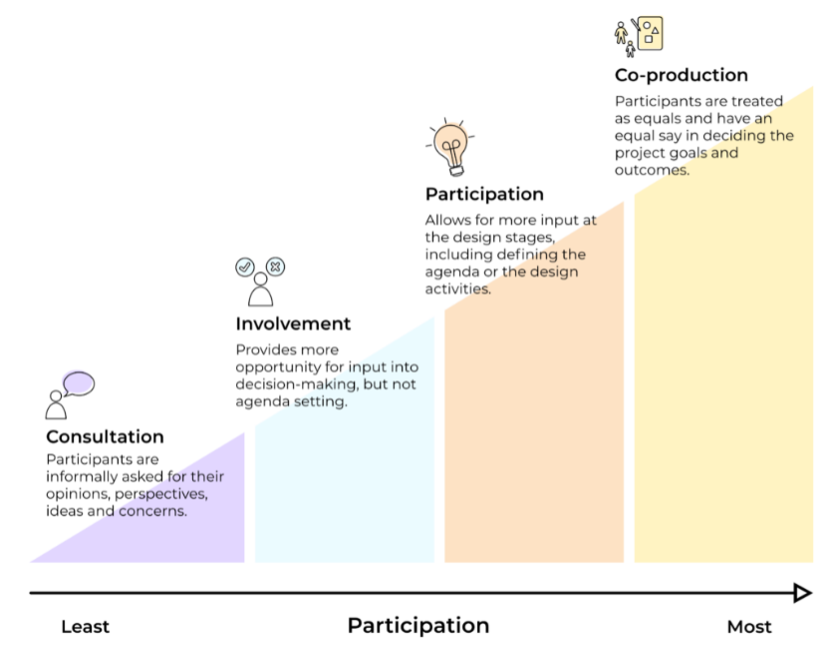
Credit: Passio
By using this model to categorise the involvement of everyone working on the project you can understand more about what sort of approach to take, meaning no assumptions are made and that everyone is able to speak about their needs on the project.
A great example is the ACCESS consortium- a programme designed to support and engage marginalised populations in complex and challenging environments (e.g. scenarios where humanitarian aid is required such as post-earthquakes or in refugee crises) to claim and access comprehensive sexual and reproductive health (SRH) information and services. The DEPTH team were part of this consortium, which saw multiple people come together from various nations, sectors and forms of expertise. The consortium had many layers because it involved lots of different organisations and staff, from those with more strategic input to those deployed operationally in-country. Being part of the consortium and seeing these layers as different communities meant that each has different motivations, interest and opportunity to be involved. The consortium leads (IPPF) were brilliant at asking how people wanted to be involved - not assuming that everyone wanted or needed to be part of everything - and using this language to ensure the right people were in the right room at the right time. Being part of such a large ‘cog’ in the consortium was also interesting because there were times when I noticed I wanted more of a consultation style role over an equal partnership and vice versa, based on how much time, interest and ability to input I had. Using a co-production model for this was helpful to understand where we fitted into the wider project, to clearly define roles and responsibilities, and also see where we had more or less influence.
2. It’s ALL about power
I came to academia from a domestic abuse charity, and lots of our conversations there were about power: power in an individual sense (e.g. an individual’s power over another) but also about power in a more structural sense, relating in particular to sexism and inequality, and increasingly racism and ableism.
Being aware of the power you have on a project is key when thinking about service user involvement. Constant reflection on issues such as whose voices are privileged, who is making decisions, who is being heard the loudest, or what assumptions are being made is so important to ensure that your involvement is not simply replicating power structures in society but is actively working to challenge and/or dismantle them.
This is best described as the difference between “doing with” over “doing to”, as in the model below:
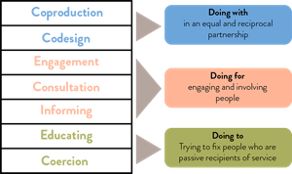
Credit: NCVO
But how do we find ways to talk about power and become aware of ways it is being used in our PPI?
One place conversations about power are happening is part of decolonisation work developing in academia. The DEPTH team discussed decolonisation across their work, challenging what is being taught to students and how this teaching represents the world. Lots of this work is about power - who has the power to tell stories and whose stories are heard. It is important to build in time to reflect on how involving people in projects can replicate problematic power structures and how to challenge them. Some people are critical of decolonialisation work and it’s definitely not a panacea, but it offers a useful place to jump in to thinking about privilege and power for others.
3. Project managers can uphold problematic power structures
Project management is essentially creating a structure to get something done. We might think “we’re just doing project management - what does racism, sexism, ableism and so on have to do with us?” But it’s important to remember that structures aren’t neutral: within the structures we create, the policies and processes we write, and the tasks we carry out, power and privilege exist. So even administrators, project managers and other support staff need to reflect on how the bureaucracy around a project could replicate or encourage oppression and marginalization of those involved in the research.
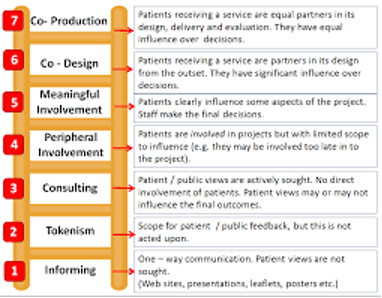
Often we don’t think about how things like a project plan or a budget can have longer term ramifications on co-production. But these are exactly where we should be thinking about service user involvement! For example, if we are writing a budget we may not have built in money for travel for service users or childcare costs, which may block people’s ability to participate. Or we may make our timeframes too tight to truly involve people, practicing tokenism rather than the time needed for co-production (see graphic below).
4. Find ways to make power more transparent
All sectors have specific problems relating to power. In academia, issues around authorship are some of the most prominent. Writing papers (authorship) is a huge part of the role and prestige of an academic. However, deciding who is first author on a paper (and the order of the authors names) is important, and credit for authorship can be an area where power obscures participation.
As part of their PPI guidelines, NIHR (a big research funder) encourage consultation, collaboration and co-production with research participants and offer frameworks of how to engage people to take on more ownership of the research. But how do you balance issues of power here and make it more transparent?
One way the team have made power more transparent is by creating “authorship guidelines”. These are a really useful guide to talking through these issues and establish who would like to collaborate, thereby shining a light on how power works and ensuring we are able to talk about it and negotiate a more equal and equitable partnership with co-authors, who may be research participants or experts from NGOs and may be unaware of some of the rules around authorship or discouraged from asking for due recognition.
5. The DEPTH Approach Works.
The ‘DEPTH approach’ is the teams’ formula to involvement within health research. And after seeing it in action, I can confirm it works! I witnessed the team working on our current project “Routes: new ways to talk about covid for better health” which has a focus on Gypsy, Roma and Traveller communities, and migrant workers in precarious jobs, and their experiences of Covid-19 and healthcare
The DEPTH approach includes a framework around how to galvanise communities to come together, share their experiences, analyse the results and co-produce recommendations for how healthcare could work better to centre their needs and priorities. The team developed an approach for how to involve those with lived experience on the team and as co-researchers (even in a project with such tight timelines), a series of insightful questions to ask during a mapping phase, and use their links and networks to reach out to a huge range of people. Involving communities is always complicated, but the DEPTH approach is a thoughtful and considered approach to how to co-produce health research which has been honed over many years of expertise within the team. The insightful results we are seeing and engagement by GRT and migrant worker communities within the project shows how successful this method is.
Conclusion
Participation at every level can be powerful, but the most important thing is to be transparent about what type of involvement people can expect - and its limits. This means people can give informed consent to take part in research as they truly know what they are signing up for, it shines a light on power (and where it’s problematic), and it is best practice for working in partnership.
I started this work in the women’s sector, and came across the most wonderful group of survivors of domestic abuse who had created a “ladder of involvement” to show how services can involve their clients. It seems only fitting that as I returned to their work as inspiration for this article, I realized that it was a student at LSHTM that helped create it all. How fitting that my two worlds have come together at the intersection of how we place people at the heart of their own care.

2021 was a busy year, for DEPTH and for researchers and communities worldwide. Here are some numbers that summarise our in-DEPTH work in2021...
1
New research project, Routes: new ways to talk about Covid for better health. Focus on Gypsy Roma and Traveller communities, and migrant workers in precarious jobs. This participatory research is funded by the NIHR Public Health Policy Research Unit. The project responds to the Health and Security Agency need for urgent information on barriers and opportunities for improving health services relating to COVID-19 community prevention and response. Check out our brand-new webpage for more information.
137
Number of organisations and individuals contacted as part of our Routes project work, across mapping conversations, interviews, dialogue sessions and stakeholder conversations.
3
Major funders for our participatory DEPTH research: UK Government FCDO (ACCESS: Approaches in Complex and Challenging Environments for Sustainable SRHR), NIHR (This Sickle Cell Life) and UK Government NIHR/DHSC (Routes: new ways to talk about Covid for better health. Focus on Gypsy Roma and Traveller communities, and migrant workers in precarious jobs). Across these projects, we are working in dialogue with communities as well as with policymakers, researchers and advocates.
14
Points in our preliminary guidelines for equitable academic authorship in collaborative health research. We built on good-practice guidelines from the International Committee of Medical Journal Editors (ICMJE), the British Sociological Association (BSA) and Committee on Publication Ethics (COPE) to recognise the specific needs of authors in co-production contexts, including research conducted with non-academic collaborators. You can read our guidelines, for free, here.
2
Finalist nominations for the Royal College of Paediatrics and Child Health &Us ‘Voice Champion Award’. Dr Alicia Renedo and Dr Sam Miles were shortlisted for their work with children and young people, ‘championing their voices to inspire students and health workers at the London School of Hygiene & Tropical Medicine’. The nominations and shortlisting were run by young people. You can read more on our blog.
8
Talented research degree students undertaking doctorates with DEPTH staff: Prima Alam, Casey-Lynn Crow, Julia Fortier, Weiqi Han, Erin Hartman, Mary Mbuo, Marthe Le Prevost (recently completed) and Maritza Lara Villota.
1,278
Total number of followers of our @DEPTH_LSHTM and our @ThisSCLife Twitter accounts. Check out our feeds out if you’re not signed up for daily updates, news articles and research findings.
90
Number of days we had to wind up a huge consortium project. ACCESS (Approaches in Complex and Challenging Environments for Sustainable SRHR) was axed without warning by the government in spring 2021. We nevertheless developed exciting outputs to share from our consortium work, available here. You can also read a summary of the project from our partners at IPPF (International Planned Parenthood Federation), here.
2
Strategy days to practice teamwork initiatives, discuss DEPTH priorities and plan our research strategy.
5
Total number of canine DEPTH team members. Gus and Ziggy are Sam and Laura’s puppies, while Bertie, Colin and Pepa are honorary doggie members!

We hope you enjoyed reading our 'Year in 2021'. Watch this space for new developments in 2022...
Our latest DEPTH blog comes from LSHTM PhD researcher Weiqi Han, supervised by Professor Cicely Marston. Weiqi has just won best poster at the 2021 Research Methods e-festival for her work on using photo-elicitation to understand the lived experiences of sexuality of young people with physical disabilities in China. Over to you, Weiqi…
‘I really enjoyed my time at the 2021 Research Methods e-festival last month, hosted by the National Centre for Research Methods and methods@manchester. Around 80 sessions were held over five days, with more than 130 speakers offering diverse perspectives on the festival’s theme: innovation, adaptation and evolution of the social sciences. The e-festival was brought together by a common interest in interdisciplinary approaches within and across the various social sciences. It was web based and was highly interactive. Attendees could join sessions via live video streams, take part in community discussion boards and network with other scholars.
I was so excited to win best poster at the festival. Currently, I am in the qualitative data collection stage of my doctoral work. I am honoured and grateful for this recognition, and I hope that it draws more attention to studies on the intersection of sexuality and disability.
For many years, people with disabilities have encountered societal stigmatisation and oppression, which often causes them to suppress their sexual lives and sexuality. People with disabilities are often seen as asexual and thought to be incapable of embodying sexual emotions and desires. The transition from adolescence to adulthood is a time of instability, experimentation and exploration in various areas of life, most importantly in relation to sexuality. In the context of China, where this study will be based, 85 million people live with disabilities, and approximately 8 million of them are young people between the ages of 10 and 19 years. Everyone has a right to sexual and reproductive health, and young people with disabilities should not be denied this inalienable right simply because of their disability.
The study seeks to explore young people (age 18–24) with physical disabilities’ qualitative accounts of their lived experiences of sexuality while transitioning to adulthood in China. Accordingly, a phenomenological approach to qualitative research will be utilised that focusses on the essence of the individuals’ lived experiences. Data will be primarily collected through photo elicitation interviews to centre the knowledge, voice, and lived experiences of young people with physical disabilities.
People with disabilities are rarely given the opportunity to share their experiences and desires about their sexuality and intimate lives. Research on disability and sexuality cannot be carried out without the participation of people with disabilities. People with physical disabilities have almost always been represented in a negative light in the visual realm. To enhance the participant-led understandings of experiences of sexuality and disability, I decided to utilise a method designed to ‘give a voice’ to the participants and allow them to talk about their experiences. Specifically, I will use photo elicitation in conjunction with semi-structured interviews to gain a ‘phenomenological sense’ of the importance and meanings that the content of the photos holds for the participants while allowing them to relate and share their issues, experiences and concerns.’
Thank you for your guest blog Weiqi, and we look forward to learning more about your project in this historically under-researched field. Watch this space!
You can contact Weiqi for more information on [email protected].
DEPTH team members collating research themes
New term, new research! We’re very excited to publish our latest article: ‘Reimagining authorship guidelines to promote equity in co-produced academic collaborations’, open access in Global Public Health. This piece brings together our thoughts on academic authorship from our recent ACCESS project on sexual and reproductive health and rights (SRHR) for marginalised populations, with our thinking on knowledge co-production from the project ‘This Sickle Cell Life’, a sociological study of young people’s experiences of paediatric to adult healthcare transitions
The call for papers for a special issue of Global Public Health on ‘(Re)imagining Research, Activism, and Rights at the Intersections of Sexuality, Health, and Social Justice’ offered us the perfect opportunity to crystallise some of the discussions we had and are still having as a research team about health co-production, academic research, authorship, and social justice. We take collaboration and engagement very seriously in DEPTH here at LSHTM, and felt that established authorship guidelines, while excellent benchmarks for ethical research and publication practices, aren’t always fit for purpose when it comes to co-produced work with different stakeholders. As we reflect in our Discussion:
There are numerous structural barriers to full collaboration that have an impact on authorship. The structural barriers to collaboration in general can be revealed in decisions about authorship – they are highlighted in who makes authorship decisions, and who benefits from them, and the structures and conventions that support and entrench inequities and devalue collaborative in favour of competitive working.
In light of these tricky contextual norms, we found numerous questions that needed unpacking: who is an author, and what do they contribute? When does a person’s place in the acknowledgements change to place on the author list, and when should it? How might we think more deeply about academic products and knowledge so that we do not inadvertently help supress voices that are already less heard? These voices are often less heard in academia because of the structures and customs of the academic system, so what impediments can we sidestep while acknowledging we still function within that system?

The result of our discussions is the article, which starts to explore how we might more explicitly pursue recognition of co-produced contributions to academic research. One way to hold ourselves and each other to account in equitable ways of working is through authorship guidelines, which we hope will prove useful as a jumping-off point for others engaged in collaborative work – especially with practitioners, activists, or non-academics, whose contributions and knowledges don’t always fit neatly into academic ‘boxes’. Having reflected on who tends to be disadvantaged by the current systems, we suggest that spending time thinking critically (and sometimes painfully) about these positions and relations can help to scaffold authorship norms that are fairer and more transparent.
You can read the whole piece here, free and open-access. But in this blog I wanted to highlight our authorship guidelines specifically. They are amended from existing excellent offerings of ICMJE and BSA, and move beyond them in that here we incorporate more explicit attention to different stakeholder contributions, and also to co-produced outputs. These are both themes that are long overdue more sustained reflection, and in an academic context of ever-increasing cross-disciplinary and cross-country collaboration and co-production with communities, we hope they prove useful for other researchers out there.
Take a look at our suggested authorship guidelines and see what you think – and reply to this post if you have suggestions for improvements or any other comments:
- The nature of academic publication processes and authorship conventions should be explained to all partners so that the meaning of authorship and involvement is clear to all parties regardless of university affiliation or discipline.
- The project research/writing team should list details of expected papers early in any sub-project, including expected authorship and author order (especially first author).
- The rationale for authorship and author order should be transparent. All authors must make a substantive contribution to the intellectual content of the publication.
- Non-academic project partners should be invited to co-author the work, with plans in place early on about how to handle suitable contributions. Level of input required must be discussed and agreed early on to ensure clarity on how authorship is allocated.
- Contributors whose contribution does not in the final product meet the criteria for authorship should be named in the acknowledgements. Named individuals must be informed so that they can withdraw their name if they wish.
- Where used, translators/interpreters must be named in the acknowledgements.
- Lead author must draft the paper, with input from other authors, and be responsible for submitting the paper and making any revisions in response to referee comments. The lead author must not submit any paper without the agreement of the named authors.
- All academic publications should contain a statement about the contribution of each named author.
- The PI must approve submission of academic articles from the project and must be named as author if criteria for authorship are met.
- Academic journal publication must be supplemented with publication of findings in other channels to ensure inclusive dissemination (e.g. tweets, policy document, media article, public workshop).
- The particular needs of members of the team should be considered in arranging publication strategy (e.g. need to gain experience of lead authorship). However, any named author must fulfil the requirements for their authorship position.
- Sole authorship will not generally be possible or desirable within the project because of the collaborative nature of the work and our recognition that knowledge is co-produced through these collaborative relationships.
- Consider adding the consortium or project name to all work with numerous contributors who do not meet the criteria for authorship and listing key contributors to the paper in the acknowledgements.
- In the event of any disagreements or confusion about authorship or author order, please refer to these guidelines within the writing team. If there is still confusion, please request assistance from the PI as the question may need to be referred for a wider discussion and/or the guidelines may need to be clarified.

In uncertain times, it was a real morale boost to receive some good news from the Royal College of Paediatrics and Child Health (RCPCH). The RCPCH ‘& Us’ team, who advocate for and involve children, young people and families in health services, recently told us that DEPTH researchers Dr Alicia Renedo and Dr Sam Miles from LSHTM were nominated for the RCPCH & Us Voice Champion Award.
The Voice Champion Award is a youth-led award recognising adults that go over and above their job role to work with RCPCH &Us to improve services with children, young people and families. The nominations were all anonymised and reviewed by young people from RCPCH &Us, who created criteria and a scoring system, then worked virtually together to review and discuss the fantastic nominations.

Alicia and Sam were not only thrilled to be nominated but also impressed by the youth-led nature of the nomination and award process. Putting young people at the heart of health services participation is key to how we work in DEPTH, so the RCPCH & Us Voice Champion Award feels like a real reflection of the values that we prioritise in DEPTH, too.
This Sickle Cell Life is an NIHR-funded research project that explores the voices and experiences of young people with sickle cell as they transition from paediatric to adulthood, and adult healthcare services.
Project Research Lead, Dr Renedo, says of the nomination:
“This was excellent news for the DEPTH team. We admire the work done by RCPCH &US, and they are a role model for participation, so coming from them, this nomination felt very special.”
Project Principal Investigator and DEPTH Group Director Prof Cicely Marston said:
“I’m so delighted to see Alicia and Sam recognised in this way. They work really hard to make sure our participatory work is inclusive and their work with young people on this project has been brilliant.”
We feel very honoured to be nominated, and thank all of our collaborators and colleagues for their role in making This Sickle Cell Life happen. You can read an ‘Evidence’ brief of This Sickle Cell Life by NIHR here.

Some of the This Sickle Cell Life collaborators (Top row L-R: Patrick Ojeer, Ganesh Sathyamoorthy, Sam Miles, Nordia Willis, Alicia Renedo, Andrea Leigh. Bottom row L-R: Cicely Marston, John James, Siann Millanaise. Photo: Anne Koerber)
Continuing from Part 1 of our Q&A last month, here’s Part 2 of our Q&A with Emma Sparrow from &Us at The Royal College of Paediatrics and Child Health.
This interview focuses on working with young people in a tricky year when it comes to participation. We asked Emma how RCPCH &Us have managed to carry on with engagement activities since Covid…

Adapting and engaging in a pandemic
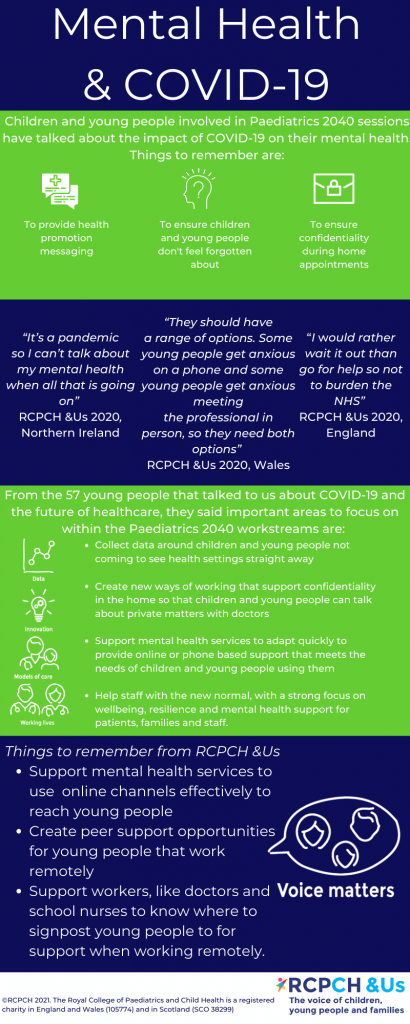
Emma: We had to look at all of our projects and decide which ones are appropriate to carry on, because we had some that were about very sensitive topics that in-person would have been challenging, and would have needed a lot of support and aftercare – for example complex respiratory illnesses. We looked at those and thought, you know, what, there’s a pandemic going on, which includes respiratory illness, now’s not the time to be phoning people up or talking to them and saying, ‘what do you think about this?’ and ‘what you think about that?’ First we did a wellbeing assessment on our workstreams and agreed which ones we were going to park for a bit, based on a welfare context. Then we spoke about what the missing gap in provision might be, because everybody is going to suddenly do everything the same and we don’t want to duplicate. We actually didn’t go as quickly as some of the other organisations to put out loads of new children and young people-focused information about COVID. What we did was pull together existing information on COVID and put it into a place that was easy and clear for families, parents and children and young people to see.
We wanted to give children and young people a meaningful role and we had to be creative
One of the things that we wanted to do was give children and young people a meaningful role. We asked: what are the gaps? Something that came up from paediatricians was that they were really worried that children and young people wouldn’t be going to their regular appointments anymore, so could we create a child health diaryfor them? So we did, and that’s still getting downloaded now, which is really cool. It’s something a bit more creative for them to write down their questions or things that have happened that are good. A doctor came to us and said ‘we want to thank our children and young people for taking part in the covid effort and not coming in and not playing outside, so can you create an E-card?’ So we created e-cards for thank you and birthdays, and last month 5,000 of those were viewed.
We picked up on children’s and young people’s concerns
As time went on we worked with lots of other groups, virtually. Lots of Teams, Zooms, and all that kind of stuff, to find out: what’s happened for you with health during COVID? What are your appointments like and what are you missing? What’s the information like? We picked up concerns from children and young people about the fact that COVID information wasn’t targeted at them. It was for adults. It also wasn’t giving a positive message about children and young people, so they were seen as the problem rather than part of the solution. There were also significant gaps forming around mental health support. That led us into a couple of new projects focused on COVID, but specifically from children and young people’s points of view. One was about mental health in a crisis, where we wanted to children and young people to tell us where they’re getting their mental health support and where are the gaps. Another one is working with young people to try and get a press conference for young people, because they’re not allowed to ask questions at the government press conferences, you have to be over 18 – excluding a whole group from having their questions heard or having a role. So we’ve been working with other charities to call for a press conference to answer questions from children and young people.
We got young people involved in reviewing evidence on patient experience of COVID
Finally, we realised that there were thousands of studies being done on COVID. The RCPCH had clinicians coming together to review which studies were being published on children and COVID, which got me thinking that actually there was also thousands of studies being published of what young people had said. Lots of charities were asking their children and young people about the impact of the pandemic, and then publishing the results. And we just wanted to give young people a chance to also do what the adults are doing: so if doctors can review scientific journals about COVID, young people can review a patient experience of COVID. We pulled together a group of a small group of young people and over 12 weeks, invited them to look at about 20 different published studies of around 60,000 children and young people’s voices, say, from cancer patients, mental health experiences of young people, children and young people or young carers, across the UK.
And they did what we do in our world – they conducted some thematic analysis, they explored the key trends, they developed them, they then created eight different topics that came up, and they slotted in the data, with a ‘for’ and ‘against’ for each topic. Topics included things like mental health and family dynamics, employment, education. They wanted to make it make a difference to the NHS, and the NHS at the moment are writing recovery plans on how to how to restart the NHS. So they’ve boiled all of that work down and they volunteered over 100 hours doing this project over about three and a half months. They’ve turned the three priorities they have developed for the NHS into posters. The posters include the priority, the problem, the solution, the impact, a quote and some stats. Since launching, the recovery plan priorities have had about 28,000 Twitter impressions. You can read more about the COVID Book Club findings online.
The work has elevated the voice of children and young people – and made people understand they have a lot to say
Emma: We also hosted a debate with doctors about whether paediatricians should be thinking holistically or medically during COVID, because for children and young people, it’s about their mental health as well. That project just feels so different from what we’ve done before. We had to really think through safeguarding and wellbeing, so we didn’t overwhelm the young people who led it. This project very much felt like we were actually paralleling something that was going on in the academic part of the college, and doing the exact same thing, but for children and young people, which felt very different. It has elevated children and young people’s ability, both in the college and in the sector. And it’s really made people understand that they have got a lot to say, and they understand what’s going on, and have a lot to offer.
So on the whole, we’ve managed to find a way or find a tool or find an approach that makes it fun and entertaining and interesting and focused on them rather than the topic sometimes.
The good thing about having to change our work is that we’ve been more connected to RCPCH wider internal projects. The benefit of voice has been seen in a different way. And for us, we had to take that opportunity and run with it – we’ve had 200 new children and young people involved during the COVID pandemic, who have between them completed over 330 hours of volunteering.
Voices are being heard and the professionals are engaging more
Emma: We give advice to people that are starting out on a project or want to talk about PPI [patient & public involvement] and I’ve had so many more requests over the last three months for people that want that advice. And I think it’s because children and young people’s voice is now seen differently. They’re really seen as being integral. There’s so much further we could go, there’s a million other things we could be doing that are even more innovative and creative, and increasing their reach, but you’ve got to start somewhere.
Barriers to participation – too much time online but also digital exclusion
Emma: There’s different barriers and challenges according to which audience you’re coming from. For children and young people, one of the challenges that they’ve said to us is that it’s really overwhelming that everything is online. We’ve really got to understand that because whilst we think we’re doing something fun and exciting, and it’s online for an hour, they’ve already had school online, for some of them health appointments online, mental health appointments, and counseling online. They’ve had zoom calls with friends and family, they’ve tried to keep fit online. And then we’re coming at them with another online thing. Another challenge for them might be: maybe I haven’t got somewhere confidential and private to do online stuff where people aren’t listening in. Or maybe I haven’t got a good device. So we’ve really looked at the challenge and been as inclusive as possible. You can join our online sessions on phone, you can do it on WhatsApp, you can join via video, you can have no video. You can use the chat, or you don’t have to use the chat, you can do it by email if that’s better – it’s all your choice. For us it’s a challenge because we’re having to run four or five different tech options for a one-hour session. But it’s about understanding that not all children and young people want to be on video, not all children and young people have got a device that lets them Zoom. Maybe all they’ve got is a landline, which means they can phone in.
The challenge for participation and engagement is don’t get complacent and think that your games and activities can all work with everyone seeing everything, because they can’t. It’s about inclusion. And that comes from children and young people saying: I might be sharing my laptop with five other people in my house, so I can’t use Teams at the same time, but I will phone in because I’ve got a mobile. We’ve had to really think it through. Another challenge is always remembering whatever you’re talking to children and young people about might be overheard. So don’t put them in positions that makes them disclose stuff that actually might not work well in their family environment. We’ve worked hard to create safe spaces, and to work with each group that we’re talking to, to make sure we understand what their space is like at that moment. Because you can’t start a conversation about money and poverty, when their parents are listening and they might feel that they’re being judged or that the young person feels like they’re judging their parents or living environment.

How can we make it fun? How can we make it inclusive?
Another challenge has been how we can make it feel fun. If you’re using devices for presentations, or for school, we don’t want to be like school on your computer. In the back of our heads we’re always thinking let’s not overwhelm our children and young people, they don’t have to come to the project if stuff’s going on. So we’ve really been conscious about trying to understand what people might be going through. And then to think about things like don’t drink or eat when you’re on camera, because not everyone has got enough food in their house. You would do that in the meeting room, but if we were in the meeting room, we would have given them food and drink. Whereas for us on camera, we’re being really careful about stuff like that. So I think that there’s some challenges. The one that we’re looking at now is where we would normally do community outreach to reach people who aren’t connected to any projects. That will be a challenge and we need to think about how best to reach out to that cohort. But no challenge means that it’s the end and we’re not there yet! It just means that I need to think harder about how I’m going to get past it.
I knew the COVID studies review would give young people a platform that they’ve never had before. But how can you possibly do that safely? If I was in the room, I’m able to see their visual cues, I’m able to unpack things over lunch, I’m able to stop the session and do something entirely different. I spoke to a friend who’s a youth worker and she said: ask the young people, they’ll tell you what works for them, so we did, and they knew all the answers and helped shape the project throughout. In the end they decided that we couldn’t do all of the studies. We found 33 but they said that they could only manage a certain number but that’s cool. At every stage I just kept checking in with them. They will tell us what works for them. It’s co production even in that sense.
What tools can we use for remote working with children and young people?
The first thing I would have to say for anyone about to do is go and talk to your information governance manager. Because whatever you think might be able to be used might not be able to be used for lots of different reasons. One thing we used is Trello , because the young people said for the COVID studies review they wanted somewhere where they could collaborate on documents, but we can’t use Google Docs because of a GDPR issue. I’ve never used anything like that before with young people. It’s so good. They could ask questions and comment on each other’s documents. But they could also see really clearly what was happening at what stage and what they could add to if they had a bit more time. I’ve been trying to find a voting app online, because that is key to so many of our projects, to be able to anonymously prioritise five or six different things. And Menti allows you to do that. You don’t have to put any personal data in, you just get given a code. And then they’ve got lots of different voting tools that you can use. Having a virtual whiteboard is really important as well, like JamBoard. But going back to inclusivity, if we’re using JamBoard, and I’ve got two people that phoned in, I will take a screen grab of it and then WhatsApp it to them so they can see it building. And it’s keeping that in mind as well, to make sure that you’re not inadvertently excluding someone because they haven’t got the same software in front of them.
Overall, I think we keep adapting, learning and changing to the meet the needs of children and young people engaging with us through the pandemic, as we learn new digital tools or approaches and learn from the group. It’s been an opportunity to really relearn everything you have always done and to reflect, update and adapt which has been hard at times but so rewarding when you see the outputs and outcomes.

Attendees at the participatory dissemination event for This Sickle Cell Life with DEPTH at LSHTM and RCPCH’s &Us (Photo: Anne Koerber)
Contacts
To find out more about the RCPCH &Us programme or to access their free resources and support go to www.rcpch.ac.uk/and_us or contact [email protected], and follow them on twitter @RCPCH_and_Us.
You can read about the RCPCH & Us collaboration with LSHTM on ‘This Sickle Cell Life’ here.

We were very excited to meet with Emma Sparrow from The Royal College of Paediatrics and Child Health. Read on for Part 1 of 2 blog posts that cover all things engagement, involvement, and PPI…
We began by asking Emma to explain her role, and how she and her team approach child health and engagement.
Part 1: How do we engage with children and young people and amplify their voices?
Improving child health is more than just paediatrics
Emma: The Royal College of Paediatrics and Child Health (RCPCH) is a charity, but as a Medical Royal College, it helps to support the specialism of Paediatrics. We’re slightly different to other Royal Colleges because we are the Royal College of Paediatrics and Child Health, rather than the Royal College of paediatricians. So it means we can get involved in the whole child health agenda, which is obviously much bigger than just paediatrics. The RCPCH &Us programme is the network for children, young people and families to help inform and influence all of the work of the College. It gives them a place to have their voice and space to say what’s going on for them and what could be done to improve child health services. Our approach is to get them involved in that – it’s not just somewhere to chat, it’s somewhere to actually get involved in and progress social action. For us it’s like a network approach where we try to get as many children and young people and families involved across the whole of the UK at all ages. This year, our youngest person involved is aged four, and we go up to age 25.
We focus on children and young people’s voice and having them involved as volunteers or project members or giving views, but we also recognise that sometimes we will need to involve their advocates as well, whether that’s parents or carers. So we do ad-hoc work with parents and carers, but our primary focus is making sure that children and young people can get involved in the work the college is doing. We also ask what might be some of the challenges in child health, that they’re keen to explore and do something about with us?
People ask what children and young people think about something… We turn the questions into games and activities and take them out on the road
Emma: Our approach is a bit different to most places. At RCPCH &Us, we work in three different workstreams. One is our roadshows and consultations. We get questions from loads of different people about what do children and young people think about something – for example at the moment I’ve got questions on what do young people think about virtual health appointments, and what do children young people think about mental health experiences? What do children and young people think about how their data is used? There’s lots of different questions that come into us. We’ll turn these questions into a set of games and activities and take them out on the road, so that we can go and speak to as many children and young people as possible in as many different areas as possible, with as many different experiences as possible. It’s about us being out there with them, rather than expecting them to fill out a survey or a questionnaire or attend something with people that they don’t know. Our roadshows might operate through schools or youth centers or playgroups or outreach. Or we might speak to children in care groups and carers, or speak to children and young people who are patients: we’ll speak to them outside their outpatient appointments, when they wait to see their clinician, or they might be inpatients.
We bring young people together for day-long ‘challenges’ or for long-term projects
The next approach is challenges. These are ‘tasters’, because children and young people don’t necessarily want to sign away their lives to a project for three years, they might want to just see what it’s like. We’ll bring them together for a project day, where they’ll come in not really knowing that much, and then learn all about a topic, they work with data, and come up with solutions and then present it at the end of the day. This is a bit like the project that we did with you at LSHTM last year – This Sickle Cell Life.
The final approach for us is long term projects focusing on a specific area, with children and young people signing up to join that project team.

Developing workshops in the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
Children and young people can participate in a way that works for them
Across our approaches, you could be a young person or child that just wants to tell us something in a conversation, that’s perfect. Or maybe you want to try something you want to do a challenge or maybe you want to do a project, but you don’t need to do all three; children and young people can come in and out as it fits for them. We really want to make it an opportunity for them that they feel is meaningful, and that fits their life rather than fits my nine-to-five work life. It includes lots of weekends and evenings, and lots of doing things in lots of different ways. But for us, that’s important because it means that we get more children and young people involved who might not have been involved before, across different ages and backgrounds.
The other bit that is different is the way that we approach diversity. So we also make sure that any project we’re doing has children and people from three different groups. One is universal, so they’re all just children or young people, because that’s who they are. Then we have a group where they’ve got specific experiences that might change the dynamic for them, for example they’re young carers, or they’re Gypsy travelers, or something that binds them together with an identity. The third group is specialists, who have the health condition, for example asthma. That explains the way that we try to deliver our work by bringing together all three groups to have a full set of views, ideas and experiences.
How do adults respond to your approach, and the way you centre children and young people?
You’ve always got people that are your allies and they’re brilliant for amplifying what’s going on. You can send them something and explain it to them and you know they’re going to get it straightaway and get it out. And then you’ve got the middle group who know that it’s important, but maybe feel stretched – overwhelmed by their work or their role. But when you can engage them in a conversation with an adult, or an organisation or a particular group of people you can see that they get it and they want to do more, but maybe the time is just not right. Those ones stay in touch, and they will get there. Then you have the people that just don’t get it at all. Either they fundamentally don’t want to get it, because they don’t think it should be happening – you’ll have people saying, ‘but why, it’s not [children and young people’s] role to say that we know what we’re doing’. Or they don’t get it because actually they’re at a point of crisis themselves, maybe in their role or their organization where it’s entirely the wrong time.
We just have to really understand that we’re going to have all of those groups, and they’re all important. They all have a role to play in what we’re doing, but the way we approach them will need to be different. So the information we give to allies and the people that ‘get’ it is what children and young people have said, and can you do something with it? Yes. The middle group, we see how we can show them the benefits of what children and young people are saying and then how it will actually support their work. For the ones that fundamentally don’t get it, we tend to talk about the legislation: there’s a statutory duty to do this, it isn’t something that I’ve just made up. It’s really important when you do engagement work that you’re aware that everybody has a different motivation as to how it will land with them, and why they might be interested. But you can learn from them and work to give them what they need. Sometimes it’s challenging but I just see it as an opportunity to share information in a different way. I have to just try harder to make sure that that it meets what they need.
I think you have to be an eternal optimist in engagement work, because everyone’s different, everyone learns in a different way, everyone participates in a different way. It’s all part of a process.

Attendees at the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
Thanks for your time Emma. Look out for Part 2 of this Q&A next month!
Contacts
To find out more about the RCPCH &Us programme or to access their free resources and support go to www.rcpch.ac.uk/and_us or contact [email protected] and follow them on Twitter @RCPCH_and_Us.
You can read about the RCPCH & Us collaboration with LSHTM on ‘This Sickle Cell Life’ here.
Here are some numbers that summarise our in-DEPTH work for 2020…

The number of partner organisations in our UK Aid-funded ACCESS consortium. We are excited to collaborate with International Planned Parenthood Federation, Frontline AIDS, Women’s Refugee Commission, the Open University, & Internews.
The new research partners within the ACCESS SRHR (sexual and reproductive health and rights) consortium. We are looking forward to working with colleagues at LSHTM Uganda and HERD International, Nepal.

The number of citations of our piece in The Lancet, Community participation is crucial in a pandemic. In it, we lay out steps governments and health bodies must take to ensure citizen participation.

The number of words in our final NIHR report, This Sickle Cell Life. You can learn more about the findings from our project here.

The number of sickle cell patient and carer experts with whom we co-produced This Sickle Cell Life. We recently collaborated with them to present study findings to London NHS Trusts.

The number of new followers to our @DEPTH_LSHTM and our @ThisSCLife Twitter accounts. Check them out if you’re not signed up for daily updates, news articles and research findings.
The number of hits on our tweets in 2020 from our DEPTH Twitter feed. If you don’t follow us already, now’s your chance!

The number of links to other articles, profiles and research findings we included in our 2020 blog posts. Our team wrote about all sorts of topics, from sex and gender to the options for obtaining informed consent in lockdown.

Photo by Clem Onojeghuo on Unsplash
New year, new blog post! For our latest piece, DEPTH researcher Dr Sam Miles reflects on the journey from PhD to first academic job, and offers some advice to ECRs (early-career researchers) pursuing careers in academia. This blog has been adapted from The Royal Geographical Society ‘Postgraduate Life‘ Series, which you can find here.
I was recently invited to write a guest blog for the Royal Geographical Society about my journey to my first academic job. I don’t have all the answers – in the piece below I reflect on exactly why this might be, and my concerns probably resonate with many of you – but I do have some ideas. Many of these came about after discussions with former students, current colleagues and other early-career researchers (ECRs) in the field, and notes of my own taken over the years.
It’s not as simple as a tick-list, though I cannot tell you how much I wish it were. I just hope that these ideas can be helpful to social science students here at LSHTM and in the wider job market applying for postdoctoral or lecturer posts. I was asked to write the kind of blog post I wish I’d read when I was starting to job hunt; with that in mind, here goes.
It’s one of those truisms that finding an academic job is hard. And it really is – it feels somehow unlike finding any other kind of job, and the specific knowledge around academic job hiring processes is something you’re also somehow expected to know, maybe by osmosis. It’s no wonder Imposter Syndrome strikes so many of us. Take for example academic CVs, where longer is better. It goes against every fibre of my being to go over the 2 pages I was always told is the maximum you should fill. Even the listing of education/jobs/experience is differently ordered in an academic CV to CVs in every other job in the world. Job adverts themselves can be confusing in terms of terminology and contract type, or arcane or unclear working conditions, or freighted with acronyms without explanations. On top of this, salary, contract length and expectations of entry-level posts can be vague, missing or intimidating.
It all results in a task that feels unclear and applications that can feel rather uncertain. Usually, that’s through no fault of your own (as evidenced when you’re several applications in, facing radio silence from each institution. Are you even doing it right?) Obviously, the offer of an actual job would answer that question, but academic posts are so competitive that your empty inbox may be more of a testament to a stricken job market than your own application – and the COVID-19 pandemic has made a precarious market even worse. You will often be rejected without any feedback from the hiring institution. The standard response to requests for feedback is that feedback is only feasible at shortlist stage, but it is invariably difficulty to get to shortlist and interview if you don’t gain feedback on what you need to finesse! In the absence of clear direction from institutions, you may need to utilise a few different approaches. I’ll lay out some that I used.
Here’s what my own journey looked like: In the final year of my PhD, I applied to several lectureships. The applications I submitted were for posts that normally required a PhD, completed or near-completion. I took this to mean that they were open to nearly-there or newly-minted PhDs as much as anyone else, but have since recognised that the field of candidates is routinely so huge that many will have progressed a long way beyond this milestone. From asking more established colleagues at my institution, talking with early-career-researchers at a conference that spring, and looking out for the hiring announcements of successful candidates (people increasingly share job successes on Twitter), I realised the reality was that new PhD finishers rarely get these jobs. The market is crowded with brilliant and highly-qualified candidates. Vacancies are limited (and by some accounts, dwindling further).
It is now much more common for PhD finishers to work on one or several assistantships or postdoctoral posts before lectureships become a possibility. Even then, that post is often fixed term.

Photo by Jon Tyson on Unsplash
During my own job hunt, a Research Fellow post at the London School of Hygiene & Tropical Medicine (LSHTM) caught my eye. It required a PhD in public health or related discipline, including social sciences. Alongside my own research covering some (but certainty not all) elements of sexual health via a PhD researching the mapping of queer male relationships on location-based dating apps, I made sure I researched reproductive health, which was the other component of the post and an area where I was less experienced. The specification emphasised qualitative methods, which matched my experience, and co-produced research outcomes with communities. My doctoral research was participant-centred and I had been reflecting on making a safe space for sensitive topic discussions, but I wanted to develop this more in future work. The LSHTM post would specifically engage participatory research, so I took my knowledge of participatory action research (PAR) from my own work and brought myself up to speed on co-production and PPI (patient/public involvement) in health.
I revised (and revised, and revised) my academic CV, highlighting teaching experience as well as research outputs to date. I wrote a targeted cover letter which addressed each of the candidate specification requirements listed in their ‘essential’ list for the vacancy. I addressed each criterion only briefly, keeping the letter to the point, but then noted down longer answers to consider for a potential interview stage. The hiring panel requested academic and non-academic writing samples, so I included a published article but also a blog I had written about the Pulse nightclub shooting in Florida and its impact on LGBTQ space. I was shortlisted for interview(!) and prepared obsessively. I read articles, chapters and media pieces from the hiring team, and took them up on their invitation to produce a slideshow to present in the job interview. I tried to make sure I could highlight the ways in which my research experience matched their goals and I matched up every item in the person specification to a demonstrable activity, role or expertise. This is so key:
You need to show how you fulfil each and every ‘essential’ criteria to progress to shortlist. If you cannot show this, or don’t effectively communicate how you show this, your hiring panel will not be able to ‘get to’ other elements of your application that are lower ranking in priority.
And… I got the job! It was only a one-year contract, but with hopes of renewing this pending funding. That happened at the end of year one, and then again six months later, and again a few months later. Three years later, and I’m still hanging on. We are now embarking on a very exciting project, after which point I will again need to think about new grants, funding and tenure.
This brings me to precarity. One thing I was asked to reflect on in my blog post was worries I had when applying for academic posts. To be honest, it’s not a past tense concern: I’m funded for now, but then I’ll need to generate grant money for future posts. What started as a temporary position became less precarious, but I’ve yet to secure a permanent position, and know strikingly few ECRs who have managed it. Over half of all UK lecturers are now on fixed term contracts. I worked for several cash-strapped NGOs before my PhD and yet have never experienced precarity like I see in academia.
It’s not a personal failing of mine – nor of my colleagues, my line manager or even my Faculty. It’s the predictable result of the neoliberalisation of universities. ECRs are good value and high output, and the incredibly high requirements of REF and general institutional reputation require in turn workers who can relentlessly publish lots of high-quality, peer-reviewed research. In this context, the idea of ‘slow’ co-production in research sadly becomes a luxury, even as my colleagues and I have shown its value.

Photo by Danielle MacInnes on Unsplash
Some final tips:
- Find academic jobs advertised on jobs.ac.uk and Times Higher. Jobs.ac.uk is better in my view because it allows tighter filtering by salary level, city and discipline. You can also ask it to direct new job alerts straight to your inbox.
- Twitter is an incredibly useful tool, not just for academic networking, but for getting to know an institution and who works there (many staff now have Twitter profiles – DEPTH even has one). It’s also useful to catch job alerts from departments in case you’ve missed them on your job hunt.
- Write a blog. It’s a tip I bet you’ve heard before and probably rolled your eyes at, but it’s true. Writing your own blog as a PhD student is invaluable. I may not keep up a regular blogging schedule, but writing a blog, especially at PhD level, has been useful for thinking ideas through, for connecting with other people online, for publicising my work. My hiring committee told me that they read writing samples closely to check that candidates can articulate ideas, and they judge generalist and academic writing equally. Writing a blog allows hirers to witness your skills already in action as a form of public engagement.
- My PhD supervisor, who was relatively early into their academic career themselves, was a source of invaluable advice, and I would definitely recommend asking to speak with your supervisor in your final year about your job application plans. Ask to do this separately from your normal supervision slot if that’s what it takes to really get your head in the job hunting zone. Talking your plans over with a supervisor is doubly useful if you have sent them your CV in advance for them to review or comment on.
- Your supervisor has been in your position themselves, and so their advice should be invaluable, but I also know that many supervisors haven’t been on the job market in years. Even if they have, the reality of today’s academic job market may be totally different from their understanding. They also may not have time to help you with cover letters or CVs. If this is your experience, ask around to see if another staff member – perhaps your head of department or research lead – would be willing to look over your application materials.
- Find your university careers service and book a CV appointment. Be clear when booking that you are applying for academic jobs and need guidance on an academic CV and cover letter – the advisor is unlikely to be specialist in that area but at least you’re giving them the chance to check up on the conventions in order to offer you tailored help. In my case at QMUL they didn’t have anyone relevant in-house but hired a specialist for PhD students as and when required – the consultant was excellent, and free for students.
- Check out websites like The Professor Is In and The Thesis Whisperer. Both include fantastic tips. The LSE careers blog includes interview guidance.
- Take some precious days away from thesis write-up to rehearse how you can show your interview panel specifically how you are the best matched candidate for the role. I’m always surprised that most people I know don’t do this, which surprises me (they also tend not to rehearse conference presentations either – horses for courses, I guess). It seems obvious that the rhythms and flow of public speaking aren’t perfected on your first run through, and that goes doubly for a speech or presentation. Do I hate it? Yes. Do I force myself to set time aside for the activity anyway so that when it comes to the real thing ‘out there’ my flow mitigates my wobbly voice or mumbling? Absolutely!
- When universities hire a candidate for a post, they need to fulfil these criteria to be shortlisted and need to demonstrate their fulfilment of these criteria again in interview, so taking time to really read and think about how you match to these criteria is crucial. Think about it: you need to minimise their labour in matching up what they are looking for when it comes to interviewing their candidates. You need to prepare some of this work for them, so they aren’t having to find ways to invite you to show how you match up – because you’ve already laid it out concisely and persuasively, on the page and in person. Good luck!
Motelism, 2017
For our latest DEPTH blog we asked LSHTM researcher Kimberley Popple to share her thoughts on NGO-academic collaborations as someone who has recently moved from the former to the latter. Thank you for your insights Kimberley – lots of food for thought!
Image: Dan Dimmock for Unsplash
Evaluation, Evaluation, Evaluation
Back in January this year I made the move from practitioner in the NGO world to becoming a researcher in the academic sector. I wanted to combine the skills I had developed in Public Health research with my knowledge and experience of programme implementation in the field. It seemed to me that there were obvious synergies and opportunities for practitioners and academics to work together to improve global health. Certainly, from my own experience, the projects that I worked on could have benefited from drawing on people with specialist skillsets in data collection and analysis and with the time to conduct literature reviews, produce evidence maps, and test the change pathways that many of the programmes were built upon.
Before moving into academia, I worked on a large portfolio of grants in Sierra Leone as part of the Ebola response. Most of the data we collected was used solely for routine monitoring and evaluation of interventions at the project-level. Its purpose was to track progress against set indicators and to report on spending to funders. As a result, collecting data that could be easily quantified was prioritised, and quantitative data was assumed by funders to show a greater impact than qualitative data. Further, qualitative data tends to fall within the remit of the accountability teams – it is used and relied upon but not as an indicator of impact. In the Sierra Leone scenario, success of an intervention was often measured by a high number of medical consultations or a large number of attendees at a meeting, rather than focusing on data related to quality of services or patient satisfaction. I remember one example of a gender-based violence (GBV) project in Freetown which was categorised by the funder as “underperforming” as the target number of survivors had not been reached. The fact that that the women who had been reached had received high quality support across the GBV spectrum of services was seemingly less valued.
In Uganda, I worked on a maternal health project which introduced a client-exit survey for women to participate in at the hospital after receiving maternity care. However, the survey was administered by NGO staff who were working with the marginalised populations, and in close proximity to the medical staff who had provided their care. There was little recognition of the power imbalance between interviewer and interviewee or the desirability bias that might be present as a result of the women’s fear of negative repercussions from medical staff.
Evaluations were often seen as a tick-box exercise for donors and their design was fairly rudimentary. By the time the evaluation report was written, the programme had already moved onto the next phase to align with strict funding cycles. This left little room to reflect on lessons learned and engage in a process of iterative programme design. A recent systematic review has highlighted the lack of evaluations conducted on epidemic responses in humanitarian and low-income settings, with only one tenth of responses evaluated and with large gaps in quality, content and coverage of evaluations, limiting the ability to improve future responses.

Image: Dan Dimmock for Unsplash
Is the landscape changing?
Over recent years, the international development sector has intensified its focus on evidence-based programming and evaluation. Many NGOs have increased their research capacity with dedicated departments and research staff (for example Airbel Impact Lab at International Rescue Committee, and the Response Innovation Lab at Save the Children), giving them the expertise and space to test out new formats for implementation, and to ensure programming is based on the latest evidence of what works.
New funding streams have emerged for research in the humanitarian field, such as Elrha’s R2HC programme, and there is donor pressure to evidence learning and use data for decision-making. Donors like the UK government’s Foreign, Commonwealth & Development Office(FCDO, formerly DFID) have developed more in-depth guidance on how to develop and use evaluation frameworks to measure impact and ensure accountability, with requests to include qualitative indicators in logframes.
What can academia bring to the table?
So, is there still a role for academics to play in supporting the work of NGOs? I believe there can be, particularly in the evaluation of complex interventions. Universities train public health professionals who often go on to work in the NGO sector. Expert knowledge of process and outcome evaluations can be drawn upon to test change pathways in Theories of Change. Systematic reviews can be performed by academics with fewer time and funding constraints, reducing the need to reinvent the wheel every time to search for the latest evidence. As academics, we can add our voice to campaigns as advocates of change. And the humanitarian health sector can harness specific skill sets in conducting clinical trials and in disease modelling. My sense is that as both sectors continue to develop and evolve, it will be important to continue to reflect on the value of academic-NGO partnerships for global health.

Image: you-x-ventures for Unsplash

Self-testing swab. Photo credit: Anne Koerber, LSHTM.
The COVID-19 pandemic is requiring home-testing in large numbers, and this process raises questions about the ethics of informed consent. In our latest blog, DEPTH member Dr Catherine McGowanreflects on a route to informed consent and suggests how governments, healthcare groups and institutions can maintain informed consent in a time of crisis.
A key step in any research project involving human participants is gaining informed consent. COVID-19 has disrupted research work around the world, and it will continue to do so for many more months. In this ever-changing pandemic environment, important research must continue. However, this work still requires researchers to think carefully about how best to obtain consent remotely.
Photo credit: IEEE Spectrum
Researchers carrying out various population surveys are sending COVID-19 tests by post and encouraging people to self-test. Self-testing kits are a good example of a process that reminds us of the need to think about consent. Research participants must provide informed consent to participate in research, particularly when it comes to population surveys involving biological sample collection. Information governancein the European Union and the UK has changed considerably with the implementation of the General Data Protection Regulation (GDPR), which does not allow for presumed consent in most cases – so when it comes to a process like home testing, for example, the data gathered cannot legally be collected or processed without gaining explicit consent from research participants.
In 2017 we carried out antibody testing amongst non-Ebola infected healthcare workers (HCWs) who had returned from West Africa following the 2014/16 Ebola outbreak. We posted test kits to HCWs throughout the UK and the Republic of Ireland, with samples returned via post. When it came to getting informed consent, face to face consent was not feasible, we could not waive consent and nor did we feel comfortable presuming consent. In the interests of best practice we also wanted to make sure that participants had all of the information they needed in order to consent fully – and be able to reach us, the project PIs, with any questions they might have. Ultimately, we decided to recruit participants via email but first they were asked to work their way through the consent materials electronically, and to explicitly indicate their consent. Once participants had consented they were asked to complete a short questionnaire and to provide their postal address so that we could send out the test kits. At the conclusion of the study we emailed participants to let them know the results of their antibody test and included a link to a survey asking about their experience of consent. Our findings, as well as a description of the design of the consent process is described in our paper which you can read for free in Journal of Public Ethics. We asked participants how much of the consent material they read, how informed they felt and if they preferred online to traditional face-to-face consent.
The results were very interesting: Participants indicated a high level of engagement with the consent materials, with 67% reporting having read all and a further 20% having read ‘most’ of the materials. All participants indicated feeling completely (78%) or mostly (22%) informed about the purpose, methods and intended uses of the research, as well as what participation was required and what risks were involved. Overall, participants reported an overwhelming preference for online consent. Their longer free-text responses suggested that they were predominantly attracted to the convenience of online consent, including the leisure to read the consent materials several times, and the ability to engage in the consent process at a convenient time/place. Free text responses also supported online consent for our survey, but participants indicated that were the study more complex or were it a clinical trial they would prefer to have a face-to-face element.
Self-testing kit. Photo: Anne Koerber, LSHTM.
Obtaining consent in lockdown
What can this study tell us about the research based on COVID-19 home-testing that is happening now? Well, it is our hope that as researchers aim to continue their work online, they give careful thought to what informed consent is in the current circumstances. Our paper describes how to obtain informed consent electronically and in a way that we have found to be acceptable amongst our research participants, but this might not be appropriate in all cases.
We also hope that Public Health England puts in place a robust framework for the pandemic to ensure adequate consent is still sought and obtained for any research. It is in times of crisis that abuses may be allowed to happen. Even with the best intentions, researchers may act expediently and may overlook best practice in their hurry to conduct the research and obtain results. In disaster settings, corner-cutting in ethical research practices are more likely, but this is also when participants are most vulnerable and may feel less able to challenge research practices that feel inappropriate. Our own studyhas shown that there are easy and acceptable solutions for obtaining informed consent. We hope that researchers currently developing population surveys using self-testing methods will give some thought to developing acceptable solutions to obtaining informed consent. We must continue research activities without forgetting our professional, ethical, and legal obligations to those who make our work possible.

Photo copyright: Catherine R. McGowan. Photo consent from healthcare worker.
Recruitment information for This Sickle Cell Life participants (Photo: Anne Koerber)
Our latest blog by DEPTH researcher Dr Sam Miles takes a break from coronavirus research to explore the themes of co-production and collaboration in our recently completed project This Sickle Cell Life. Read on to find out more…
Regular readers of this blog will know that our work in DEPTH (Dialogue, Evidence, Participation & Translation for Health) includes thinking about how we involve different communities in health research. Today I’m writing about This Sickle Cell Life, a recently completed qualitative research project that talks to young people about their lives and experiences of having sickle cell disease. I should add that some of what I’m writing about is based on team discussions and reflections. We’re writing this up in more detail with our co-authors and I’ll keep you posted on how it progresses.
I got involved in This Sickle Cell Life with Professor Cicely Marston and Dr Alicia Renedo when I started here at LSHTM in 2017. Funded by the National Institute for Health Research (NIHR), the project explores how young people experience transitions in moving from paediatric to adult healthcare services. This includes for example how our participants experience GP surgeries, scheduled hospital visits or unscheduled (i.e. emergency) trips to A&E. We also explored the personal and day-to-day experiences of young people living with sickle cell disease. We were aiming to answer questions including: What is the relationship between a young person with sickle cell and their doctor, and how does this change if you move away from home for college, university or work? And why do young people with sickle cell sometimes delay going to the emergency department when they have a sickle cell pain crisis? (Read this excellent overview by Sickle Cell Society for more on pain). We then cast the net wider to think about family, school, sex and relationships.
Our aim was to offer a much-needed sociological picture of how a young person with sickle cell navigates their life and their future, to mirror the more extensive clinical and quantitative research that has been published about the condition. That’s not to say that sickle cell research is exactly a crowded market – Professor Simon Dyson, who has made brilliant sociological contributions over many years, has rightly noted the lack of sickle cell research compared to other chronic health conditions, and how social, economic and ethnic determinants play into this marginalisation:
‘…impairment is primarily socially created by environmental factors, consumption patterns and accidents and not by genetic disorders.’ (Dyson 1998: p.123).
Sickled cells (Photo: Wikipedia Commons)
Co-production
Fieldwork was already expertly wrapped up by Alicia when I joined the project, but I got to be part of the really interesting results analysis, discussion and dissemination work, including an engagement event with the public which in turn led to some fantastic community projects of its own. You can read more about the work here, but what I’m going to focus on in this blog was the role of ‘co-production’ in the project: put simply, that means working with different ‘kinds’ of people to produce research that is a collaborative effort. Co-produced research recognises that expertise is held by a range of people rather than only the ‘usual suspects’ (in this scenario, academics or clinicians). Advocates of co-production hope that the research findings developed are more rounded-out and take into account the ‘embodied’ knowledge of people who are living the journey themselves (see Renedo et al., 2018 for more).
One of the distinctive features of This Sickle Cell Life was that it was co-produced with two young sickle cell patient experts and a sickle cell parent/carer expert from the outset. All three have extensive knowledge of sickle cell and life with sickle cell, and already advocate for healthcare improvement in their own lives. They were involved long before I was – right from the project planning and application stage before funding was granted, in fact. They were also paid for their time. Partnering with these three experts added a very important facet to the research we conducted. There is a lot of talk in public health research about ‘PPI’, or patient & public involvement with healthcare. In the NHS, the motto ‘nothing about me, without me’ represents one way in which patient involvement is rationalised. Funders and grant-giving bodies are (rightly) keen to see meaningful involvement with the communities (sometimes also called beneficiaries) who are most relevant to the research being done. Co-production can also shine a light on the power imbalances that often happen in a traditional researcher-participant relationship in social sciences research which can reinforce all sorts of unhelpful hierarchies and prejudices.

Documenting the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
In our project, we agreed with our patient experts that it was particularly important that their voices were heard, because they contributed expert knowledge of their bodies and their own health conditions, as well as helping us at the findings stage of the research, highlighting themes that were most pertinent to improving healthcare environments for people with sickle cell. We further argued at every stage (to colleagues, institutions, sceptics – anyone who would listen basically) that our involvement processes needed to be considered, balanced, and properly thought-through – lip-service involvement doesn’t help any party and it is not in the spirit of meaningful participation. We wanted to amplify less-heard voices and hear stories from our patient experts and carer experts because their analysis of their own, and others’, experiences of sickle were invaluable. Our collaborators’ input contributed a different side to more traditional qualitative research; as a team, we worked to interpret the data and draw out the implications for practice.
The highlight of the project for me was not just the valuable findings that came out of 80 interviews with young people, which are research outputs of their own brilliantly managed by Alicia (which you can read for free here), but the process of co-producing research with patient experts and carers. I have discussed the idea of co-production a bit in my own digital technology and sexuality research, in which I (loosely) explored the co-production by both researcher and participant of a safe discursive space for covering sensitive topics in sex and sexuality in fieldwork research (which you can read for free here). But This Sickle Cell Life made co-production central from the start and throughout the full four years of the project; it is clear to me only now how truly different this way of working is, and the value it adds.

Attendees at the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
The winding road to publication: How expertise is framed in academia
What was interesting was how our co-produced research outputs were received by peer reviewers for academic journals. Having learnt so much from our patient experts about how their experiences reflected what our results showed us about participants’ experiences, we invited them to write an academic article with us. We did this by discussing study findings with them and inviting them to discuss these themes with us as I took notes and recordings to write into a larger discussion. It was a long process, involving lots of conversations in cafes, on the phone and by email to coordinate our different experiences and expertise.
However, upon submission several reviewers critiqued what they felt to be overly personal accounts of sickle cell. Even having noted our co-produced efforts and celebrated this ethos, reviewers still picked out patient expert passages that they felt were lacking objective research – questioning the expertise of our co-production partners who were best placed to be reflecting on the study findings. Where our patient experts told us how their experiences chimed with those of the participants when it came to hospital care or chronic ill health or family issues, and I wove these reflections into our discussion section, reviewers felt this expertise was anecdotal or somehow unscientific – as if the rest of the qualitative dataset was by contrast unobjectionable or markedly positivist, when of course it wasn’t. We were in the paradoxical position of amplifying the expert knowledge of people with sickle cell and yet that knowledge being somehow too ‘real-life’.
We were in the paradoxical position of amplifying the expert knowledge of people with sickle cell and yet that knowledge was somehow too ‘real-life’.
I have sympathy for the reviewers, too, because despite the best will of a whole range of actors to more actively incorporate a range of knowledges into academic publications, establishment traditions prevail. This clashes with what I guess I would call the out-of-place-ness of equitable authorship, which synthesises a range of voices, including those which are non-establishment and may contribute in different (often refreshingly different) ways than are standard. None of this is to say that it wasn’t a valuable experience, but it was a long one. Critical Public Health and its editors did support our approach, with suggestions back and forth, and published what we hope will be the first of several co-produced articles (read it for free here).

That leads us to one of the curious tensions in this kind of work – our collaborators are clearly experts, but they’re not academics. Does that matter? Well, it shouldn’t – especially given the UK NHS drive to centre patients and public at the forefront of research and healthcare involvement. And yet the process of publishing papers with our patient experts was not straightforward. It required different ways of working than what we were all used to, and different approaches – and that’s before we consider the lengthy journey we then had publishing our co-produced academic article, where roadblocks re-emerged.
I came to see that the key contribution of any author is their contribution to ‘the work’, and this can go far beyond typing up results or making an argument for changing UK healthcare practices in an academic article. Instead, it is about having conversations – in ways that ensure equity between all parties – and then using academics’ toolkits to package this co-produced knowledge whilst maintaining its integrity. For us, a more liberatory outcome would have been yet more unconventional than the finished piece. Maybe this would have taken us further from what makes an academic article an academic article. Well, you might argue, if you really want to publish more collaboratively, perhaps a different format would be better suited – a commentary, or an editorial, or a blog – and we are in the process of doing all those things. But this argument overlooks the ostensible openness of academic publishing to co-produced and public involvement endeavours. We’re all supposed to be embracing that ethos…aren’t we? There is work to do, it seems, in lining up expectations with conventions in co-produced research outputs.

Workshopping involvement at This Sickle Cell Life participatory dissemination event (Photo: Anne Koerber)
Final thoughts
As for the research itself, it’s been a fantastically valuable project for better understanding the health and social conditions of sickle cell. There are definitely ways we can further improve on our approaches to co-production for next time. It’s also not to say that our co-production work was straightforward or easy. On the contrary, it required constant communication between all parties to stay on the same page. But that ongoing relationship, and that time taken to gather views from around the table really ought to be how we always operate: with care, consideration and dialogue between all parties at all times. We came to define it as ‘slow co-production’, which I’ve blogged about before (we lay out what we think are its strengths in this article). It is only within the tight parameters of contemporary academic research contracts that this valuable, lengthy process feels like a luxury. I should add that the NIHR were very supportive of our approach and helped us build into our budget money to support exactly this kind of process, and they also gave us a generous timeframe in which to generate all this co-produced work.
It also encourages us to question what constitutes ‘knowledge’, who or what entities ‘hold’ knowledge (and you see it performed nowhere more starkly than in healthcare settings), and of the power imbalance between researcher and participant. Now I think twice before internalising the status quo of privilege and position in knowledge-holding (and knowledge exchange). I think more about how practical experience informs knowledge – or is overlooked by systems of knowledge and knowing – and who actually gets a seat at the table in supposedly collaborative endeavours. Cicely and Alicia have written about all of this and more, and you can read this work here, here and here.
Pursuing co-production helps us recognise the importance of prioritising equitable social science research that values all voices equally and recognises a range of expertise, rather than relying on the (often colonial, socially-structured, privileged) expertise bestowed – and often still prioritised – by academia.

Some of the This Sickle Cell Life collaborators (Top row L-R: Patrick Ojeer, Ganesh Sathyamoorthy, Sam Miles, Nordia Willis, Alicia Renedo, Andrea Leigh. Bottom row L-R: Cicely Marston, John James, Siann Millanaise. Photo: Anne Koerber)
This Sickle Cell Life was funded by the National Institute for Health Research Health Services and Delivery Research Programme (project number 13/54/25). The views and opinions expressed therein are those of the author and do not necessarily reflect those of the HS&DR Programme, NIHR, NHS or the Department of Health.
Recent social media debates have shown that misunderstandings about ‘biological sex’ are common. In our latest blog, DEPTH Director Professor Cicely Marston discusses how simplistic ideas now circulating about biological sex miss the mark – and why it matters.

Photo by Liv Bruce on Unsplash
Isn’t it the case that biological sex can only be binary – that you can only be biologically male or biologically female? And why does it matter anyway? In this blog I’ll discuss why biological sex is more complicated than many people think.
A popular way to explain the concept of ‘gender’ is to say that ‘sex is biological and gender is social’. This can help get the idea across that gender is ‘social’ – that is to say, it is something created by people, involving things like expectations, behaviours, and beliefs about masculinity and femininity. It’s true that gender is indeed social, but this leaves the idea that ‘sex is biological’ unexamined – and in some aspects in fact, ‘biological’ sex is social too.
But how can ‘biological sex’ possibly be in any way social? The basic thing to understand is that categories and labels – even words themselves – are social. For instance, if I call something a table you will know roughly what I mean. The table is real, material, and can vary: for example being made of different materials, in different sizes, and so on. We agree as speakers of the language roughly what we mean by “table”.

Photo by Abel Y Costa on Unsplash
All the word “table” reflects is what we have decided, collectively over time, counts as a table. E.g. a table generally has legs, but not always the same number. It might be raised high off the floor, or be low. Through usage, all that diversity comes to be labelled with the same word “table”.
When differentiating tables becomes socially important, language adapts, and the word “table” might be qualified (“occasional table” or “coffee table”).
In the same way, “biological sex” is what we conceptualise, as a society, as “biological sex”. It is a label used to describe a collection of indicators, biologies, and anatomies. Indicators (e.g. chromosomes, gametes), that have changed over time and with scientific discoveries. It’s not a failsafe way to know what a particular individual’s biology is in every case.
This is why we can say that the biological sex binary is socially constructed– biological sex as male or female is a shorthand for categorisations of the material world that we find useful.
![]()
Photo by hessam nabavi on Unsplash
To take the most obvious example, many people see a “biological” binary in genital shape, yet this is an imperfect heuristic. (Content warning: genital cutting mentioned below). In many places, babies are assigned to the category “male” or “female” based on the shape of their genitals at birth. However, individuals may have a genotype that appears to “contradict” their assigned sex, or that in other ways doesn’t matchthe simplified XX vs XY that we learn at school. Unsurprisingly, people who assert that biological sex is binary seem to offer varying and sometimes contradictory biological markers that they claim divide everyone in the world neatly into two categories. Is it chromosomes? Gametes? Testosterone levels? Genital appearance? Nobody seems to be sure.
“Biological sex” is a construct that helps our highly gendered society to categorise and label others.
“Biological sex” is a construct that helps our highly gendered society to categorise and label others. But why bother? The sex binary has major social significance (so much so that children with genitals less easy to read as male/female may be subject to genital cutting), and people who do not present in line with the sex they were assigned at birth, or who are not read as clearly “male” or “female”, continue to experience social disapproval, discrimination, and violence.
The idea of “naturalness” or the intrinsic/immutable binary nature of “biological sex” is important socially too. If the binary is “natural” or “biology” there’s nothing we can do about it, and departures from the typical become “disorders” rather than simply variation. Similar ideas also underpin arguments that differences (and inequalities) between men and women are biologically determined and so cannot be overcome.
The biological sex binary oversimplification does particular harm when it is weaponised to vilify or discriminate against individuals or groups who are deemed not to fit such as people not easily read as “female” or “male”, and when backwards logic is used to try to gloss over discrimination and vilification by representing it as simply a consequence of the “natural” order of things.
To summarise, “biological sex” involves not only the material but also the social. The crucial point is that the idea of a strict and immutable binary is socially constructed. The concept of “biological sex” is not inevitable because we have bodies, it is a response to how we see those bodies and how, as a society, we want to divide them up into categories. So the whole argument about gender and sex binaries is not an argument about science – however much people want to present it as one – it is an argument about classification and how we as a society choose to label people. Biological sex is social as well as material: and that matters.

Photo by Luca Vavassori on Unsplash
What do you think? Thoughts, questions – and answers – are, as ever, welcomed in the Wordpress version of this blog, available here.
Happy new year! We are welcoming back our readers with this new blogpost by DEPTH researcher Sam Miles, who was recently invited to be interviewed about sex, technology and cities for the Urban Political podcast. Read on to find out how it came about…

Sam: As well as working with my DEPTH colleagues here at LSHTM on sexual and reproductive health and rights (SRHR) for marginalised populations, and on the voices and experiences of young people with sickle cell, I have for a while now researched the relationship between sex and sexualities, digital technologies, and space. It’s work that I started for my PhD in 2013 and every year the themes it throws up feel even more relevant – how people find social or sexual relationships, how personal safety operates online and offline, what community means for LGBT+ people, and how we integrate (or don’t integrate) technologies into our daily lives.
I was recently invited by The {Urban Political} podcast to give an interview on dating apps and urban geographies. The {Urban Political} produces podcasts on ‘contemporary urban issues with activists, scholars and policy-makers’ that aim to advance our understanding of urban environments and how we might make them more democratic. They wanted to discuss my research on the relations between online dating apps and the production of urban space, especially with regards to sex and sexualities. I said yes because I was so intrigued by the questions presenter Dr Markus Kip posed:
Do apps like Grindr and Tinder make the city a more loving place? Do they make dating more safe for women or trans people? And do they cohere greater acceptance of queer cultures, or the opposite?
These are important questions. When put to you by someone not in your head, as it were, they have the helpful effect of sharpening focus on what is really at stake when it comes to the reality (and future) of digital technology and the welfare of sexual minorities.
People’s lived experiences are important. Thinking about the consequences of changing physical environments through the use of dating and hook-up apps beyond simplistic readings of ‘good’ and ‘bad’ offers us a real opportunity to think critically about what these platforms mean not just for individual users, but more widely for society, community and geopolitics.

That’s not all: in the podcast we also discuss what app companies do with the data that users provide (whether willingly or unknowingly), and what ethical boundaries are being tested in this kind of data sharing – as well as the ethics of app use itself. I’ve argued before that locative media technologies have grown at such a rapid pace that mutually-agreed social codes for use are yet to catch up with the development of these sophisticated platforms, which can lead to clashing expectations between users. I believe these (perfectly valid) tensions will be replicated and amplified across a wide range of social networks and ‘smart’ technologies in the near future as digital technologies become progressively more integrated into our daily lives.

As for the question ‘what needs to happen at an individual, collective or technological level to make online dating more useful or pleasant?’, there are any number of answers, and for me none of them are definitive. It’s become clear over recent years that dating apps are not an alternative utopian world, free from the ugliness of ‘real’ life – numerous reports of racism (special mention for #KindrGrindr), femmephobia and fat-shaming on just Grindr alone exemplify exactly that. But maybe there is space for a future of sociality, solidarity and support for sexual minorities who network online. We already see these kinds of networks in action in queer organising, online communities, and support groups at various scales and in various guises. There is no reason why dating and hook-up apps cannot similarly be collectively co-opted to embrace more ‘promiscuous’ socialisation to combat loneliness, more political solidarity with a range of queer identities and livelihoods, and more support for sexual rights agendas, whether they be PrEP provision or sexual & reproductive health rights. We can make it a 2020 resolution, can’t we?
You can listen to the podcast here, and check out other Urban Political podcasts here. There’s plenty to choose from, from the Hong Kong protests to heritage vs. gentrification.

This article was adapted from Sam’s blog post on Sexuality & the city.
In our latest blog post, DEPTH researcher Dr Alicia Renedo gives us an overview of her experience delivering a short course on participatory research at Kyoto University School of Public Health.

Kyoto streetscape. Photo: Alicia Renedo
The short course consisted of two full day workshops (day 1 Professor Pranee Liamputtong and day 2 Dr Alicia Renedo), which included a combination of mini-lectures, reflective discussions and participatory group work by students from Kyoto University. Research degree students from LSHTM also attended the course at Kyoto and presented some of their own participatory research projects
Professor Liamputtong from Western Sydney University delivered an engaging session on the theory and methods of PAR (participatory action research). PAR emphasises involvement of participants in the research undertaken and encourages participants to shape the research undertaken. The day started with an inspiring introduction into the philosophy behind PAR, which drew upon the pioneering ideas of Brazilian educator Paulo Freire. Students learned about the importance that Freire’s work has had on the theory and practice of participation for social change and health improvement. In particular, Professor Liamputtong challenged students to think about how Freire’s concepts of ‘radical love’ and ‘conscientization’ can contribute to more equitable research. This is a type of research that challenges the status quo by engaging ignored and silenced voices and addresses the problems marginalised communities identify as central to their everyday life.
Professor Liamputtong contextualised PAR within the wider debate about decolonising research methodologies. She drew on Linda Tuhiwai Smiths’ work to make an excellent case for the need to stop conducting research that takes away the knowledge and livelihoods of communities and suppresses their identities.
This introduction to the theory and philosophy of PAR was followed up by an overview of different creative PAR methodologies, from body-mapping to photovoice. We also learned about the personal skills PAR researchers need to develop; reciprocity, self-reflexivity, respect, self-awareness, humility, and compassion amongst others.
On the second day, Dr Renedo encouraged students to think critically about participation in health. She gave on overview of the body of work she’s developed with Professor Cicely Marston focused on understanding how community participation and patient involvement in healthcare research works in practice: what works, why and how? She started the day with an introduction to work they have developed on theorising participation and using participatory approaches in health research. Their work has addressed important evidence gaps on participation in health by developing critical theory on undertheorized aspects, which are also neglected in practice. In this first session, students learned about the importance of space in making participation successful and inclusive, and about the role of temporal, social and material aspects of participatory space in influencing participants’ ability to negotiate their rights for quality health and to mobilise for better health.
In this session, students also learned about how social relationships and research practices at the core of participatory research shape the identities of participants, that is how participants see their role and capacity to influence. Dr Renedo closed this first session with a discussion about the social production of new forms of knowledge through participatory processes; what happens when the technical knowledge of researchers and healthcare providers interacts with the knowledge brought by communities?
In the second session, Dr Renedo stimulated group discussion around the guiding principles for participatory research. She introduced students to guiding principles for ensuring participatory research is ethical and inclusive to deliver bottom-up solutions for the communities we are working with. Students were tasked with planning a participatory research project with vulnerable communities. Before they started, Dr Renedo warned students about some of the potential risks of participatory research, for example, community disengagement, mistrust and reinforcement of pre-existing inequalities and power hierarchies.

Kyoto University campus lunch. Photo: Alicia Renedo
In the afternoon, Dr Renedo presented a case example of DEPTH participatory research project co-produced with sickle cell disease (SCD) patient advocates (patients with SCD and carers of patients with SCD). Her session was followed up by presentationson PAR conducted by LSHTM research degree students: Asmae Doukani, Stefanie Fringes and Chris Obermeyer.
Asmae Doukani gave a talk about her participatory research journey and reflected on her personal learnings about meaningful user involvement in the development and evaluation of digital mental health interventions. Chris Obermeyer gave an overview of his grassroots participatory research involving communities in improving PrEP promotion in Ukraine. Stefanie Fringes helped students think critically about how to do participation with young people as research partners in the context of HIV in adolescent health.

Alicia would like to give a special thanks to Ayako Kohno and Teranee Techasrivichien, from Kyoto University School of Public Health, for inviting us to participate in the workshop. She adds:
“I was truly inspired by all presentations and by Kyoto University students’ critical insights into participatory research. The workshop stimulated truly collective learning. I look forward to continue conversations and see how the students can draw on the learnings from the two-day workshop in their own research.”
A recording of the two-day workshop will be available via Kyoto University’s website. We will add a link to these resources when they are ready.
Today’s blog is very topical because LSHTM doctoral researcher and DEPTH member Shelly Makleff recently attended the SVRI Forum 2019 in Cape Town last month to present a co-produced project by LSHTM, IPPF/WHR and Mexfam that highlights the potential of sexuality education as a strategy for preventing partner violence. DEPTH director Professor Cicely Marston is co-PI. Their presentation is entitled “Preventing intimate partner violence among young people – a qualitative study examining the role of comprehensive sexuality education”. Now let’s hear a little more about the project…

We wanted to know if sexuality education can help prevent partner violence. The London School of Hygiene and Tropical Medicine (LSHTM) partnered with IPPF/WHR in New York and Mexfam in Mexico City to try to find out. We have promising results that we’ve begun to publish. Below we share some of our key findings.
 Mexfam taught a 20-hour course to high school students on a weekly basis for one semester. We evaluated this course through a longitudinal study with nearly 300 students. Using observation, surveys, interviews, and focus groups, we found four main ways in which sexuality education seems to contribute to intimate partner violence prevention and response.
Mexfam taught a 20-hour course to high school students on a weekly basis for one semester. We evaluated this course through a longitudinal study with nearly 300 students. Using observation, surveys, interviews, and focus groups, we found four main ways in which sexuality education seems to contribute to intimate partner violence prevention and response.
First, encouraging critical reflection. The course provided a space to share experiences and debate beliefs about violence. For example, questioning whether jealousy and possessive behavior were signs of love, or rather, forms of violence. One young woman said:
The health educator made it very clear to us that if your partner really loved you, they would accept you as you are. They wouldn’t be telling you ‘don’t dress that way’ or ‘I don’t want you to talk to him.’ That is a type of violence.”
Participants also said the course helped them rethink gender norms. One young man told us:
My classmate said that the man has to work, and the woman should stay in the house. It made me think. I think you need to give freedom to both people in a relationship.
Second, building assertive communication. Participants said they became more comfortable talking about relationships and sexuality as the course progressed. They also shared the information from the course with friends and family, intervened in violence around them, and some left possessive relationships.
Third, promoting care-seeking behavior. Health educators emphasized the right of young people to receive care, and provided information, support and referrals. Students told us they felt more prepared to seek care if it became necessary. Indeed, the percent of participants who knew where to seek support for violence more than doubled over the semester.
Fourth, ongoing training and support to health educators. This is crucial so they are prepared to address conflict in the group, encourage critical reflection, and create a safe space for discussion.

Copyright Mexfam, 2019
Based on the three-year project in Mexico, we have recommendations for implementation and policy that can be found in our briefing paper. Here are some highlights:
-
First, communication with participants can continue after an intervention ends, to encourage access to support and care in the long term.
-
Second, sexuality education should engage teaching methods and participatory activities relevant to participants’ lives.
-
Third, such courses should aim to shift gender norms, avoid heteronormative bias, and highlight forms of non-violent behavior.
-
Finally, school authorities should formally support such interventions and ensure that teachers and other staff are trained to address school-based violence.

In conclusion, we suggest that relatively short-term sexuality education has real potential to help prevent intimate partner violence. The findings reinforce the importance of working in schools – which are strategic both as settings for violence and for its prevention.
You can read more about our findings here:
Makleff S, Garduño J, Zavala RI, Barindelli F, Valades J, Billowitz M, Silva Márquez VI, Marston C. “Preventing intimate partner violence among young people – a qualitative study examining the role of comprehensive sexuality education.” Sexuality Research and Social Policy (2019). https://doi.org/10.1007/s13178-019-00389-x
Briefing paper: “Preventing intimate partner violence among young people– The role of comprehensive sexuality education.” Advancing Learning and Innovation on Gender Norms (ALIGN) (2019).
Stay tuned for further academic papers and a series of three policy briefs, the first of which can be found here: https://www.ippfwhr.org/wp-content/uploads/2019/10/policybrief.pdf
You can also follow Shelly on her new Twitter account, and check out our ongoing DEPTH research on Twitter.
What do you think? Thoughts, questions – and answers – are, as ever, welcomed in the comments section below this blog.
In a new blog comissioned for BMJ, DEPTH team member Professor Cicely Marston and Dr Suzanna Francis argue that neglect of STIs and infertility undermines family planning programmes worldwide.

Copyright: LSHTM
Why do people still not use effective contraceptive methods?
One reason is that many women and their families in low- and middle-income countries fear the most effective contraceptives can cause infertility. A conventional response to this is that people simply need more information to put them on the right track – that women who, for instance, are using injectable contraceptives simply need reassurance that any fears of infertility are unfounded.
But what if the risk of infertility in some lower income countries is all too real – but the real cause is hidden? This, our paper argues, may well be happening with infertility caused by undiagnosed, asymptomatic STIs.
Chlamydial infection in particular is an important cause of tubal factor infertility. So infertility caused by undetected, asymptomatic chlamydia may well be widespread in areas where it is prevalent – including among women who have recently stopped using contraceptives.
All of this may contribute to a sense that it is the contraceptives causing the infertility – simply because their use coincides with less or no condom use, and undetected STI infection.
An indicator of the scale of the threat STIs pose to women’s fertility comes from recent work (here and here) in South Africa, showing a major, uncontrolled chlamydia epidemic among young people. It seems reasonable to assume that this problem, and any resulting infertility, is not confined to one country.

Copyright: LSHTM
We hope our commentary will encourage more research into the global prevalence of STIs and the degree to which the associated infertility could be undermining people’s trust in family planning programmes. Counterintuitively it is possible that by addressing fertility problems in programme settings, fertility may even be reduced as more people trust that they can use contraception without experiencing devastating infertility.
More broadly, we call for research and programmes that address women’s own priorities as a starting point to develop sexual and reproductive health programmes that are more attractive and win people’s trust.
To address complex problems, programmes and research must be co-produced with the communities concerned, and break down disciplinary boundaries such as those between family planning and STI prevention and treatment.
Crucially, programmes must address women’s right and desire to control their fertility in the fullest sense – in other words having children when they want them as well as avoiding births when they do not. In high fertility settings, infertility – so often personally devastating and socially stigmatising for the people affected – may not even be considered a problem by funders. This needs to change.

Copyright Daniel McCartney
by Cicely Marston, DEPTH research group (Twitter), and Suzanna Francis

This post was first published online at BMJ Sexual & Reproductive Health on September 26 2019.
You can read the full paper here in BMJ Sexual & Reproductive Health, open access and free to read: Neglect of STIs and infertility undermines family planning programmes
In our latest blog, DEPTH researcher Sam Miles discusses his latest publication for new social science collection The Geographies of Digital Sexuality. Sam’s chapter explores the practices of men seeking men on online dating apps and argues that these practices can be categorised into different identities, or ‘typologies’, of user.
 I was invited last year by Andrew Gorman-Murray and Catherine J. Nash to write a chapter for their new book, The Geographies of Digital Sexuality. I thought for a long time about what to write about. My work has been moving over time from queer male technologies and fieldwork ethics to sexual behaviour, and from there to sex and sexuality more generally, as our new ACCESS project at London School of Hygiene & Tropical Medicine develops. I’m still fascinated by technology, sex and relationships, but looking globally at some of these relationships in very different contexts – marginalised populations, challenging settings, and complex geopolitical environments in the global South.
I was invited last year by Andrew Gorman-Murray and Catherine J. Nash to write a chapter for their new book, The Geographies of Digital Sexuality. I thought for a long time about what to write about. My work has been moving over time from queer male technologies and fieldwork ethics to sexual behaviour, and from there to sex and sexuality more generally, as our new ACCESS project at London School of Hygiene & Tropical Medicine develops. I’m still fascinated by technology, sex and relationships, but looking globally at some of these relationships in very different contexts – marginalised populations, challenging settings, and complex geopolitical environments in the global South.
We know that gay and bisexual men in Europe and north America are a comparatively privileged sexual minority (although MSM – men who have sex with men, but don’t identify as gay or bisexual – are often less privileged), especially compared to lesbian, bisexual, and transgender people. The lives and experiences of a wider range of people need further amplification – especially given common misunderstandings about technology use in socioeconomically disadvantaged settings; people are often surprised to hear that smartphones are used almost everywhere in the world. This includes within seriously deprived settings, where it may be the single most important object for a family’s livelihood or income. That does not mean it is not also used for communicating, partner-seeking, or pornography in any number of these settings.

Photo by Martin Tod, licensed under CC BY-NC-SA 2.0
Nevertheless, one of the things that people still ask me a lot about when they hear about my PhD and its research into smartphone dating apps is about people’s behaviour online: things that people complain about seeing again and again. It’s as if there are a list of the ‘usual suspects’ to be wary of when using dating or hook-up apps, from the ubiquitous time-waster (‘talk, talk, talk, and yet never agrees on concrete plans to meet up) to the catfish (‘Amazingly good looking but interested in me!’, or ‘keen to meet but there’s something weird about the photos’). It provoked new questions based on online identity: Could we sketch out different ‘types’ of dating app user? Would those ‘types’ translate between queer and heterosexual? Do different apps host different types?
My qualitative fieldwork suggested that male-male apps contained ‘types’ that were far more specifically defined, and more commonly recognised by a whole range of users, than anything I was reading about being theorised elsewhere, so I looked into it further and developed three ‘types’ of user: the Embracer, the Timewaster, and the Minimalist. Whilst the vignettes I write in the chapter are fictional, they are amalgamated from a range of real-life users I spoke to, augmented by the profiles of other users that my participants discussed repeatedly (and usually in strongly positive or strongly critical ways). These profiles build an interesting picture of different modes of use for a market-dominant app like Grindr or Tinder. These ‘types’ of user, and the strong feelings they provoke in others, also speak to an argument I bang on about a lot: that the social codes of these GPS-enabled apps have yet to catch up to their digital sophistication. The result is user enthusiasm for what these platforms can offer in meeting new people – especially important for sexual minorities – tempered by real frustrations about other people not taking the app seriously, or taking it too seriously, or just not reflecting the user’s desired path to encounter.
Even more fascinating perhaps is the finding that the Timewaster – an app user who is keen to chat, seemingly reciprocates interest, and yet keeps postponing a date or other physical meeting, seemingly content to exist only in cyberspace – is almost universally criticised by users. Yet many of these same users sometimes exhibit precisely this behaviour themselves. This paradox serves to emphasise that we must not think of ‘types’ or user typologies as somehow fixed, but instead flexible categorisations that users might adopt, consciously or not, at different times in their app use over time. You may not see yourself as a time-waster because it’s not a trait you think is very attractive, but that doesn’t mean that sometimes you’re not that person to another frustrated user.

The picture built up by this qualitative work is one of seriously mixed feelings. Users characterise their time using online partner-seeking apps with as much ambivalence as enthusiasm. Thinking more about what the categories I have sketched out above might mean for online partner-seeking, and how social and/or sexual connection happens (or doesn’t happen) online can help us to think about larger questions far beyond the scope of dating apps. These include who we are when we’re online, and why that still feels ‘removed’ or disembodied from what should by now be a more taken-for-granted, hybridised digital-physical reality.
The chapter is called ‘Going the Distance: Locative Dating Technology and Queer Male Practice-Based Identities’ and you can read it here, or view the full book listing here.
This post has been adapted from Sam’s original blog at Sexuality & the City.
How do researchers go about interviewing people about sex and sexualities? To what extent do we – or should we – share our own experiences? And what kind of ‘spaces’ do these highly personal conversations fit into?

DEPTH researcher Dr Sam Miles was invited by the academic journal Area to write a blog for their outreach website Geography Directions, based on his recent article ‘“I’ve never told anyone this before”: Co‐constructing intimacy in sex and sexualities research’. In the blog, Sam explores the ethics of fieldwork in sex and sexualities research. Have a read…
The (in)famous male-male dating and hook-up app Grindr recently celebrated its 10th birthday. To mark the anniversary, a whole range of articles have cropped up variously celebrating and lamenting Grindr’s influence across the world (by which I mean literally across the world – it counts nearly 4 million active users across 234 different countries (Grindr, 2019)). What makes this generation of mobile phone matchmakers different from the online platforms that went before them, for example Gaydar, match.com, Yahoo chatrooms? Apps such as Grindr are GPS-enabled, which enables users to ‘rank’ other users of the app by proximity, ensuring that potential matches can be discovered and introduced in real-time across physical space.
Reflecting on Grindr’s first decade, The BBC identifies a ‘rocky relationship’, whilst VICE magazine explores Grindr’s relationship with identity fraud and drug-based ‘chemsex’; meanwhile, Gay Times reports that 56% of Grindr users believe they can find true love on the app. Whatever your opinion on it – and there are many – there is no doubt that this mobile phone matchmaker, along with its competitors Hornet, Scruff & Jack’d, has had a profound impact on gay and bisexual communities. These apps have also opened up new avenues for men seeking sex with men (MSM) who for whatever reason – familial, cultural, or religious – do not identify as gay or bisexual.

Grindr Stock image
The bigger question raised by these recent articles seems to be: how do dating and hook-up apps impact on same-sex and queer relationships today? This question cannot be answered by quantitative usage data alone. After all, we know that high usage does not necessarily mean high popularity. We need to explore peoples’ real life experiences in order to more fully understand the impact of dating and hook-up apps on same-sex and queer relationships.
I decided that the best way to get a detailed understanding of how these apps influence sexual and social behaviours would be to interview users about their experiences online, offline, and in the ‘hybrid’ space bridging the two, where virtual introductions result in real-life encounters. My doctoral research revealed some important findings: (1) that dating and hook-up apps play a significant role in how men now meet other men, especially within wider debates about the ‘death of the gay bar’, and (2) that the relationship between mobile phone dating app users and the people they meet can be awkward, with social cues yet to catch up to the sophistication of the technologies in use.
The sensitive nature of the research topic meant that there was an array of ethical and practical challenges for me to grapple with during my doctoral fieldwork. In my recent Area paper, I reflect on some of these challenges and explore how researchers and participants can work together to create a meaningful space that not only enables data collection, but facilitates honest and valuable conversation. I consider what the researcher’s responsibility should be for a participant’s safety in this discursive space. I also reflect on how ‘involved’ I should be as a researcher. I’m a person, not a robot, and several decades of feminist research has already explored the strengths and issues bound up in bringing ‘yourself’ into the research field (for example, see Bain & Nash (2006) and Smith (2016)). But the opposite extreme of the objective, positivist robot researcher is the inappropriately involved one, a role which would be both institutionally unethical and personally unacceptable. I therefore identified my own boundaries as well as the participants’s boundaries. The result was a co-constructed discursive space that we worked together to construct, perhaps surprisingly, in totally public venues and in one-off, hour-long interviews rather than more private or longer-term meetings. These were not ‘intimate’ spaces in a traditional sense, but nevertheless the space-within-a-space that we constructed invited app users to speak about highly personal experiences, some for the first time ever.
I also make the case for the using public places for staging sensitive conversations. The assumption that private matters cannot be discussed in public requires a rethink. Public spaces like libraries or cafes enfold within them more private spaces – not just actual booths or nooks, although these can contribute – but I’m thinking here about more conceptual spaces. These are built simply via one-to-one, in-person conversation in a space where a hubbub of background talking, or the hiss of coffee machines brewing, provides a backdrop to conversation that can be very productive.
Finally, when it comes to dating and hook-up apps in particular, I suggest that people are particularly keen to share their views because the social norms of dating app use are so complex and still so poorly understood. For lots of people online dating remains taboo. In this context, the chance to share their thoughts, feelings and experiences when it came to the digitally-introduced, physically-involved relationships these platforms offer may have been liberating.
Love dating apps or hate them (or both), what I hope the article communicates is that we need to talk more with users about the ways in which technologies impact on our personal lives, in order to think about the social codes developing from their use that will inform a whole range of wider contexts.
What do you think? Let us know by commenting below…
References:
Bain, A., & Nash, C. (2006) Undressing the researcher: Feminism, embodiment and sexuality at a queer bathhouse event. Area, 38, 99–106. https://rgs-ibg.onlinelibrary.wiley.com/doi/pdf/10.1111/j.1475-4762.2006.00663.x
Damshenas, S. (2019) 56% of Grindr users believe they can find love on the app, study finds. Gay Times. Retrieved from: https://www.gaytimes.co.uk/community/119691/56-of-grindr-users-believe-they-can-find-love-on-the-app-study-finds/
Fox, L. (2019) 10 years of Grindr: A rocky relationship. BBC News. Retrieved from: https://www.bbc.co.uk/news/technology-47668951
Grindr. (2019) Grindr.com. Retrieved from: https://www.grindr.com/
Miles, S. (2017) Sex in the digital city: location-based dating apps and queer urban life. Gender, Place & Culture, 24, 1595-1610: https://www.tandfonline.com/doi/abs/10.1080/0966369X.2017.1340874?tab=permissions&scroll=top
Miles, S. (2018) Still getting it on online: Thirty years of queer male spaces brokered through digital technologies. Geography Compass. e12407. ISSN 1749-8198 DOI: https://doi.org/10.1111/gec3.12407
Miles, S. (2019) “I’ve never told anyone this before”: Co‐constructing intimacy in sex and sexualities research. AREA. https://rgs-ibg.onlinelibrary.wiley.com/doi/full/10.1111/area.12550
Smith, S. (2016) Intimacy and angst in the field. Gender, Place & Culture, 23, 134–146.
Staples, L. (2019) Grindr Users Talk Highs and Lows After Ten Years of the App. VICE Magazine. Retrieved from: https://www.vice.com/en_us/article/59x83d/grindr-users-talks-highs-and-lows-after-ten-years-of-the-app-1
In our latest blog, DEPTH team members Professor Cicely Marston and Dr Alicia Renedo explain how we actually get thinking (and writing) done when everyone wants our time.

Have you tried time blocking to deal with the endless onslaught of tasks in academia? It works for us. We’d love to hear about other experiences in the comments too.
Universities are sources of endless admin and bureaucratic reporting processes (e.g. supervision contact points for overseas students, online appraisal systems). The ever-increasing managerialism and research-related admin work (ethics applications and funding reporting systems) leave little time for doing research and knowledge production activities. It is very difficult to free up time to engage in in-depth academic activities such as data analysis, and writing.
To protect ‘thinking space’ and to manage work overload, we use a very simple tactic: calendar time blocking. We use this in two ways:
- To ensure we complete all of our responsibilities (as a task checklist)
- To manage our time and energy better.
Calendar time blocking helps us meet deadlines, but also helps plan for the different types of knowledge, levels of concentration and time needed for specific tasks. For instance, in-depth conceptual work and theory development, writing, and analysis require extended periods of time and can be jeopardised by interruptions such as admin requests, emails and meetings. It works simply by treating each task as requiring an appointment to complete. You estimate how much time you will need to complete the task, and make an appointment accordingly in your calendar.
Alicia: I block Fridays as a writing day, and try to block 2-3 day per week when I need to do more intensive analysis and writing. I have chosen Fridays as a writing day because this is when there are fewer emails and requests for meetings. Because some admin work requires prompt responses, I leave tasks such as emails and form filling for times of the day when my brain works less efficiently and just before a break (e.g. lunchtime and/or end of the day before leaving the office). I try to organise meetings around these times too, and when possible I try to concentrate meetings on the same day(s) of the week. For those days full of meetings I put fewer in-depth tasks in the calendar for the little remaining time available.
Cicely: I increasingly block almost every task, even fairly small ones, in my calendar. It can be alarming to see the reality of how much time is used up in management and admin. I have several research projects that I am either leading or contributing to, so I need to have leeway in my calendar for unexpected or overrunning tasks. For this reason I only block four days (usually Monday to Thursday) in my calendar – inevitably I have spillover into the ‘spare’ day and it saves me having to rejig all the time blocks in subsequent weeks. In the unusual cases where there have been significant delays that will affect future tasks, time blocking means I can more easily see if I need to rearrange non-urgent meetings or tasks so that I can still meet deadlines, or whether I need to give advance notice that I might be late completing a task. I like it when others use time blocking because they can give me a realistic idea of when they can complete a task and I can plan my work accordingly. Writing this blog with Alicia has made me reflect that I should aim to have a weekly writing day as well as a ‘spillover’ day blocked in my diary.
Calendar time blocking helps us by protecting our thinking time; by helping avoid the situation where admin tasks interfere with the flow of ideas and reflective processes needed for in-depth academic work; and by stopping us quickly jumping into smaller admin tasks at the expense of dealing with more painful tasks, such as writing. It is easy to fall into dealing with tasks that can be completed quickly and avoid slower more in-depth ones which produce longer-term outputs.
Calendar blocking can also bring collective benefits. For instance, it helps when justifying to others why you cannot instantly respond to their requests. It can also help others organise their calendars – we often set our calendars to produce and deliver papers so that we coincide with the ‘free’ space in our co-authors’ time-blocked calendars. Time blocking also helps students know when they can access our support and this helps them plan ahead to deliver their writing work, with the assurance that we will send feedback on time.
 Tip: In outlook, emails can easily be converted into appointments or meetings. Using this means you have relevant details in your time block ‘appointment’ when you work on the task (assuming you are time blocking using Outlook calendar), rather than having to go back and search for them.
Tip: In outlook, emails can easily be converted into appointments or meetings. Using this means you have relevant details in your time block ‘appointment’ when you work on the task (assuming you are time blocking using Outlook calendar), rather than having to go back and search for them.
Do you use time blocking? Any tips about how to do it better gratefully received in the comments!
For our latest blog we are thinking about ethical issues in research. Here, DEPTH staff member Dr Catherine McGowan discusses some of the roadblocks to resolving ethical dilemmas in the public health field.

Ethical dilemmas are part of professional life. But how do we navigate these dilemmas successfully? How do we ensure that we are resolving dilemmas in a way that leaves us feeling as though we have taken the best possible course of action?
People regularly make difficult decisions in their daily lives and are accustomed to resolving ethical dilemmas based on personal reflection and consultation with family, friends, and colleagues. Resolving dilemmas in the workplace, for a public health professional, is different in the sense that decisions may affect the health and wellbeing of many people. For example, decisions about resource allocation – in a context in which the public need for services outweighs an agency’s capacity to deliver – can markedly reduce life expectancy in areas not receiving services. Making the best possible decision in such circumstances, one which promises the greatest common good, is often difficult. Yet recognising, understanding, and resolving ethical dilemmas is like any other technical competency. Training in public health ethics provides the basis for sound ethical decision-making, but how many public health professionals have received education or training in public health ethics? How often do public health professionals encounter ethical dilemmas? How do public health professionals approach complex moral dilemmas?
In our latest paper entitled Education, training and experience in public health ethics and law within the UK public health workforce we present the results of a survey of 562 public health practitioners in the UK. The Faculty of Public Health, the Royal Society of Public Health (RSPH), the UK Public Health Register (UKPHR) and Public Health Englanddisseminated a link to an online survey asking about experience, education and training in public health ethics. Nearly 40% of respondents were public health consultants or specialists; the rest were registrars, academics, directors of public health, practitioners, managers, nurses or midwives. Over half of the respondents reported encountering ethical issues on a monthly, weekly, or daily basis whilst just under a third reported that their organisation had implemented mechanisms, adopted tools, or recommended resources to facilitate consideration or resolution of ethical issues. Interestingly, when asked to indicate how they go about resolving ethical issues the majority indicated that they resolve them in discussion with colleagues or on ‘personal reflection’. That is to say: the least common way of seeking to resolve ethical dilemmas was by consulting an ethicist!
We also asked respondents how dealing with ethical issues affects them: over half questioned whether they dealt with ethical issues in the best way and a quarter reported feeling anxious about dealing with ethical issues at work. Interestingly, many respondents indicated that they enjoyed the challenge of dealing with ethical issues. Unfortunately, relatively few respondents had received training in public health ethics.
Moving forward, we believe there is a need to develop and support capacity among the public health workforce through the provision of education, training, guidance, and mentoring in public health ethics. Public health professionals should be equipped to make the best possible decisions in complex circumstances for the betterment of health, and wellbeing and equity.
Look out for our upcoming paper in the Journal of Public Health – it will be published as part of a thematic issue on public health ethics. We’ll post about it on our Twitter feed and DEPTH website, so look out for updates.

PhD researcher Shelly Makleff and Professor Cicely Marston, members of the DEPTH research hub at London School of Hygiene & Tropical Medicine, have collaborated to write a new blogpost about the value of qualitative data in assessing sexuality education.
Their piece, titled ‘Qualitative data shows how sexuality education can address social norms’, explores how comprehensive sexuality education (CSE) might influence young people’s beliefs and behaviours, via a study examining a one-term comprehensive sexuality education programme implemented by Mexfam. The researchers employed an in-depth, longitudinal qualitative approach to the research field to learn about changes as they were happening, rather than after they had taken place. As Makleff and Marston argue:
A combination of retrospective interviews with a wider range of participants and longitudinal interviews with a small number of “case study” participants can be useful: it illuminates a range of participant experiences while enabling researchers to zoom in on some of the small and gradual changes that they experience.
You can read the full blog on the ALiGN website, here.

Two members of the DEPTH team, Cicely Marston (supervisor) and Shelly Makleff (PhD student) discuss how best to present quotations from interview transcripts when writing up. We talk about how to present ‘untidy’ speech (e.g. ‘um’, ‘er’, repetition), how much to ‘tidy up’ quotes, and the implications of any ‘tidy up’.
Shelly’s interviews and analysis have been done in Spanish and the quotes she presents in the final write up are translated into English. Here we present a lightly edited version of a supervisory email interchange we thought might be useful to others.
SM: How do you clean up a transcribed quote to present it in an article? Every time I cut some words, even just filler words, should I mark these omissions with an omission marker (such as […])? Or do I have the liberty to just cut those fillers without a […], in order to create a clean and readable quote?
CM: In my opinion all cuts should be marked with an omission marker (e.g. […]). I have argued about this with a journal before because newspapers use ellipses to indicate omissions (rather than a specific omission marker that only indicates omissions). The issue is that when you do this, there is no obvious way to mark pauses in someone speaking so you would need to find another pause marker that won’t be confused with an omission marker. You could do this by writing [pause] every time, but this also makes quotes hard to read if there are a lot of pauses. When you are using translated quotations, it is less clear what to do because for instance, you might keep the translation ‘clean’ by not including every single one of the filler words (though I would recommend you keep them as much as possible where there is a direct translation (e.g. in Mexican Spanish, hesitation where people say ‘este…’ can be translated as ‘um…’ in English), or at least if there is no direct equivalent, make sure you keep the spirit of the original which might have involved hesitations).
For translations, where it is good practice to provide the original language version in an appendix, one way to get around this is to present the original language quotations with all the pause markers etc included, and then present ‘tidied up’ translations in the body of the article. If you do this, you should mention it in the methods section so the reader knows they can refer to the original language quotations. Note that ‘tidying up’ is particularly challenging when you are working in your non-dominant language, which is all the more reason to present the original language transcript excerpts verbatim.
SM: Ok, so sounds like you’d always use […] to signify every piece of cut text in the article. For a conference poster, do you think it’s ok to leave out the […] for filler words so it’s smoother to read?
CM: I would keep it precise i.e. show where you have edited – I assume you won’t cut all the ums and errs. I get quite suspicious when I see a perfect quote because very very few people speak in complete sentences with no hesitations. if you genuinely think the hesitations are unimportant in any given instance, then you *can* edit them, but make sure there is a note that you have done this somewhere on the poster, for transparency.
SM: If I’m adding clarifying info in [], do I do that instead of or as well as the words that are being replaced? In other words, would it be “So for them [the students]” or “So for [the students]”?
CM: I would go with the longer version so that it is clear what they actually said versus what is your interpretation/explanation.
SM: Can I add punctuation and make sentences to create more clarity, when the speech was transcribed as a long run-on sentence?
CM: Yes, definitely improve the punctuation – transcriptions are almost always badly punctuated, especially when the narrative includes reported speech, in which case transcribers often give up on attempting to punctuate it altogether – and to be fair it can take a while to get it right even if it is quite obvious without punctuation what the speaker has said. It is worth doing because it does make it much harder to read when transcripts not properly punctuated. If you are not sure how to punctuate the sentence from the transcript alone (e.g. it is unclear where the emphasis in the sentence was), you will need to go back to the original audio to ensure your ‘new’ punctuation correctly represents what was said.
SM: I wish there were guidelines for this! In a quick internet search, I didn’t find any, at least not that are clear per discipline. While looking for guidelines I did see an article about the diversity of perspectives among academics about how they edit qualitative quotes. One perspective in favour of editing out the filler words pointed out that if participants saw their own quote with all the filler words, they’d feel embarrassed, and it isn’t an expectation that everyone speaks perfectly but that as researchers we should present their ideas as clearly as possible in a way they’d feel comfortable with. And actually, in Mexico when we shared the transcribed quotes with the health educators, they felt embarrassed about it, joking that they needed diction classes. They even made a meme of their horrified reactions when they read their words on paper and heard how they talked (see below). For the presentation of the data, we hadn’t really cleaned up the quotes, it was mainly verbatim, but the idea still stands- the way we represented them didn’t make them sound eloquent, and that embarrassed them.

This meme was created by health educators in Mexico (Ana Karen Alameda Esquivel, Benjamín Israel Bellazetín Ruíz, Yaret Gutiérrez Cruz, Karla Alejandra Medina Alcántara) who were research participants, in response to hearing us read out their own quotes verbatim. [Translation: first picture – when they give you the results from the course you implemented; second picture – when you see the transcription of how you speak]. Presented here with their permission.
CM. I agree that if the quotes have names attached to them, the person might prefer a ‘cleaned’ version, but your quotes are anonymised and so from an individual perspective I don’t think that is too much of a concern.
Having said that, it’s true that original, not tidied-up quotations might contribute to a discourse of the ‘other’ being inarticulate. People who are looking for ways to find others inferior will likely find them regardless and so I’m not sure that compromising the integrity of the transcript will help (although I’m open to arguments to the contrary).
Overall, though, going along with the idea that there is a ‘better’ way to speak brings its own problems. Should we all speak in perfect sentences? Who determines what is ‘perfect’ or ‘best’? This is especially difficult if you are trying to ‘tidy up’ sentences that were spoken in another language than our dominant language. As researchers we should commit to transparency. Interviewers who worry about their sentences should probably listen back to the interviews – they will hear that it sounds very normal, even if they hesitate, repeat words, use filler words, reframe questions and so on. It’s important to build rapport – if you don’t naturally speak in 100% full sentences in real life, why would you do so in an interview? Being inauthentic, or struggling to present a more perfect self, may well have a negative impact on the interview overall.
What do you think? How have you handled these issues? Let us know in the comment section below. If you can’t see where, click on this article headline and scroll to the bottom.
This blog post is by Dr Sam Miles, who discusses the recent publication of his academic article ‘Still getting it on online: Thirty years of queer male spaces brokered through digital technologies’ in the journal Geography Compass.
By way of introduction, I thought I’d borrow from my latest article to give you a snapshot of what I’ll be talking about in this blog post:
I call on contemporary scholarship to demonstrate how [mobile phone] platforms offer a way into answering larger cultural questions about cruising, queer social life, and space. I conclude that these locative digital media occupy a distinctive position in the history of queer technologies and signal a shift in how gay male online spaces are both conceptualised and experienced.
In the social sciences, theories of sex and sexuality have long been tied up in ideas of space and place. There are any number of examples we can think of, from the spaces of sex work and how these spaces are regulated or policed, to the rise (and more recently, fall) of the commercialised ‘gay village’ in the global north, which is often discussed in terms of its relations with economics and gentrification.
Trying to better understand the relationship between sex and sexuality and space is important because beyond theoretical ideas, it has an impact on how a location might influence sexual identity, practices or safety. For example, healthcare interventions for sex workers might depend on a safe space accessible from their working space. Civil rights demonstrations or an LGBTQ pride parade in a repressive political environment can be read as a temporary ‘queering’ of the orthodoxy or regime by making space for sexual difference in streets normally controlled by the mainstream.
My own research has focused on digital technology and sexual practices. I have been interviewing ‘MSM’ (men who have sex with men, including but not limited to gay and bisexual men) to learn more about how recent developments in technology mean that queer male space is not just physical, but virtual too.
Geography Compass invited me to write an article for them reviewing the history of queer male online space. I think this topic is particularly fascinating is because the social sciences have long tracked physical queer spaces, and this research is widely known; less is known about how online platforms contribute to producing or re-making queer spaces. What I specialise in is locative media – by which I mean GPS enabled mobile phone apps – that are now very popular amongst MSM to network and meet others for social and/or sexual connection. These locative apps include Tinder, Grindr and Hornet, and have a huge user base around the world. Grindr alone counts nearly 4 million users per day.
I argue that the development of mobile internet over the past decade, and the GPS abilities that are now built into even basic smartphones, strongly influence how men meet other men for relationships and sex. This in turn has an impact on ‘offline’ LGBTQ venues such as gay bars or cruising sites, as well as traditional understandings of ‘queer community’ and what that might mean. As I write in the article:
Male–male locative media can strengthen and extend social‐sexual networks, facilitating meetings with like‐minded men across a borough, district, or city. This is especially true among the users for whom a queer community is out of reach because of their isolation, whether familial, social, or geographical.
Of course, being connected to other sexual minorities through an app does not automatically constitute a community, but some users do report a sense of like-mindedness, even if this does not match up with the more established ways in which we define community.
Beyond MSM populations specifically, this idea of technology redefining community, whether for better or worse (or indeed both!) is crucial to how we understand how technology mediates human behaviour. In a public health context, technology needs to be harnessed in ways which are alert to local conditions, whether that is in terms of unequal access to technology, or an affinity (or restriction) to certain kinds of communication device. At the same time, the widespread adoption of mobile phone technology – 5 billion people worldwide now have access to mobile phones – shows that digital technology ‘on the go’ will become ever more central to daily life. The job now is to extend research carried out on mobile digital technologies and sexualities to different populations to help us understand more about how these platforms will impact on social and sexual practices in the near and distant future.
You can read Sam’s article here and follow him on Twitter here.
What is the legacy of medical sociology? How has it shaped other disciplines and practices? And what is its role in challenging the status quo of inequalities in health?
These were some of the topics discussed by very talented people at this year’s MedSoc (Medical Sociology) Conference in Glasgow. These were also some of the issues that drove our aim to explore how transitions to adulthood for young people with sickle cell could be improved and how healthcare services could help support these. The conference provided a great opportunity to present our sickle cell research.
Our presentation focused on how health transitions shape the identities of young people and how this contributes to the ways in which young people develop into adult patients. Transitions to adulthood can often bring challenges, and for young people with sickle cell, the challenges often faced in education, social and emotional transitions to adulthood are complicated by their condition, and they must navigate these complex changes as well as changes in their hospital care that can bring problems as they move from child to adult health services.
There was a range of interesting presentations to choose from. Martyn Pickersgill’s fascinating talk about the dialectic between patient experience and diagnostic practice, resonated with some of our findings on the hybridisation of knowledge through the dialogue between ‘subjective’ patient experiences and ‘objective’ evidence. Charlotte Kühlbrandt’s ethnographic paper helped to shed light on the intricate relationship between citizenship/non-citizenship and patienthood/non-patienthood in the context of Roma Health Mediation in Romania. In this case, health mediation becomes correction in the production of normative forms of citizens and patients. In our case, we showed how healthcare transitions become self-disciplining ‘at a distance’ and form part of a relentless process of self-governance through which young people try to become the types of patient and citizens they ought to be.
Eva Krockow made us think about how we balance the individual versus collective good when we make choices about antibiotic prescribing.
The panel plenary, with a focus on inequalities, was fascinating. The keynote papers from Professor Ellen Annandale discussed the ‘gendering’ of health inequalities and the embodiment of global gender power relations such as the health consequences of biogenetic trade. Professor Hannah Bradby pointed out barriers faced by forced migrants across Europe, the stratification of migrant status and how this interacts with “acceptable” forms of vulnerability. Some migrants find themselves having to amplify and enact their vulnerability (mental health) to access care and citizenship status. Professor Graham Scambler’s keynote paper on “What’s Left of Class for medical sociology?” encouraged discussion about our role as sociologist activists in challenging health inequalities.
With Scambler’s call to action, I left the conference eager to continue my commitment to medical sociology and critical engagement with inequalities in health. You can keep up to date with our work in these areas via our website, DEPTH twitter account and our This Sickle Cell Life project twitter account.


This week, we are heading to Glasgow for the BSA Medical Sociology Annual Conference to share a sneak preview of our findings from This Sickle Cell Life: voices and experiences of young people with sickle cell.
Sickle cell disease is a genetic blood disorder disproportionately found in minority ethnic communities in Britain. It is a chronic debilitating condition that both causes cumulative damage to multiple organ systems, and causes acute pain.
This Sickle Cell Life is part of the work of DEPTH research group at LSHTM. The project explores how people move from using child to adult healthcare services and asks young people about their experiences of living with sickle cell. Transitioning to adulthood is obviously not just something that affects clinical experiences and so we also explore education and relationships, and ask young people what is important to them.
At the BSA MedSoc conference we will talk about how healthcare transitions shape the identity of young people, and how these transitions help ‘make’ particular kinds of patients.
Why focus on identity? Health transitions need new health knowledge and new behaviours to develop, but they also need development of self-perceptions and understandings of how a person should behave as an adult (rather than a child) patient. In this way, identities play an important role in shaping health practices and beliefs. Understanding identity development during transitions can help explain why some young people transition smoothly or less smoothly into healthy adulthood.
In our presentation, we will talk about how ideas and discourses about self-management and healthy lifestyle within healthcare today act as a way to discipline young people “at a distance”, to quote Miller & Rose (1990) and influence their behaviour. These healthcare self-management discourses intersect with demands from schools that are often not compatible. For instance, schools demand that young people excel and become entrepreneurial, competent individuals, but excelling at school is far more difficult for young people who have to spend time in hospital, or who have to rest regularly to avoid having a pain crisis. These intersecting demands can translate into conflicting “self-disciplining” identities.
For young people with sickle cell, we found that transitions to adulthood involve relentless self-disciplining and self-surveillance to try to be as healthy as possible, while also aspiring to work hard so that they can develop and meet educational and career goals.
You can follow our live updates from the BSA conference on our Twitter account, here.
Despite widespread media attention, repeated public health alerts, and the US President’s declaration of the opioid overdose epidemic as a ‘public health emergency’, fatal overdoses continue to rise.
A key factor is pharmaceutical fentanyl - a powerful synthetic opioid commonly used in clinical settings to reduce moderate to severe pain. Since 2014 illegally manufactured fentanyl, and many of its analogues, have been used to adulterate street drugs, principally heroin. Fentanyl is considerably more potent by weight than heroin and has been responsible for a significant number of fatal drug overdoses in North America since 2015.
Preliminary data released by the Centres for Disease Control and Prevention suggest that in 2016 more than 20,000 people died from unintentional overdoses involving synthetic opioids (not including methadone) in the United States. In Canada, 3,671 people died from unintentional overdose in 2017 – 72% of these deaths can be attributed to fentanyl or fentanyl analogues.

So what can be done?
Harm reduction agencies in North America have begun to distribute test-strips which, when dipped in a drug solution, are able to detect fentanyl and many of its analogues. Is this a potential answer to the overdose problem? Perhaps; but caution is required.
First, research suggests that while self-testing technologies may be accurate in a laboratory, they may be considerably less effective when used in a real-life setting. Contamination, for example with injecting equipment, is more likely to occur in a street setting than a laboratory.
Second, the test strips are only able to indicate whether or not fentanyl is present in a drug solution, they do not indicate how much fentanyl is present. In cases where a comparatively large proportion of a drug is fentanyl, ‘test hits’ taken by users to reduce their risk of overdose in response to a positive test may be ineffective in reducing the risk of overdose.
Third, while some test strips have demonstrated greater than 95% accuracy, this still leaves the possibility of a false negative in one in twenty tests of fentanyl-adulterated drugs. People may inject heroin up to five times a day rendering false-negative a fairly regular occurrence. Additionally, test strips have shown to have a low detection limit, a drug sample may test positive when a minimal amount of fentanyl is present. There is a risk that users may not consistently modify behaviour if drugs are routinely testing positive without producing the anticipated psychoactive effect.
Fourth, not all test strips are created equal. DanceSafe, a US-based public health organisation, in conjunction with the University of California San Francisco, tested five fentanyl test strips from three different manufacturers and found that four of the test strips did not detect carfentanil (a fentanyl analogue that is considerably more potent by weight than fentanyl); one test strip did not work at all.
The need to tackle the fentanyl crisis is clear. A recent drug-checking pilot carried out in Vancouver found that 90.6% of drugs submitted tested positive for fentanyl. Though fentanyl was most commonly found in heroin, it was identified in other street drugs as well, including: amphetamines, methamphetamines, crack, and cocaine.
And the problem is not confined to North America. Since 2014, six fentanyl variations have been identified in the UK, with several overdoses attributed to fentanyl occurring in the North East of England in 2017.
But should we be promoting test strips as a potential solution to the crisis?
In June 2018 Health Canada cautioned against relying on test strips alone, suggesting that other precautions were necessary to prevent overdose including: never consuming alone, consuming a lower dose - “start low and go slow”, and only using drugs in the presence of someone who is equipped with, and knowledgeable about the administration of, naloxone.
Providing appropriate messaging on how to interpret test results and their limitations is key. We must understand more about the accuracy and acceptability of fentanyl self-testing, and research should also aim to inform the development of an effective means of dispensing test strips – and associated risk-reduction measures - to those who do not regularly come into contact with harm reduction services. Education and appropriate harm reduction messaging to mitigate against the risk of false negatives alongside strategies to prevent or reverse overdose is crucial.
There is huge potential in self-testing technology but it must be used as part of a package of risk-reduction measures. The problem is clear but the answers are not.
Our article, ‘Slow co-production’ for deeper patient involvement in health care’, has just been published in the Journal of Health Design. It’s open access so anyone can read it, download it and share it. The article argues that ‘Slow co-production’, achieved by involving patients in in-depth research, can help deepen patient involvement in health care. We describe how slow co-production offers a mutually beneficial form of patient and public involvement. It promotes patient-centred knowledge and helps us to examine and reflect on the co-production processes themselves, rather than always rushing to evaluate the end product as if it came into being without a process and a series of human relationships.
The thinking behind this article was our different and shared experiences of time constraints in qualitative fieldwork. We discussed, for example, those times when we felt pressured to move on from fieldwork when we didn’t feel we had been able to fully examine the narratives that we were learning about, or the interviews we were conducting. This restriction to fieldwork research is usually required for budget and time constraints, but it can feel frustrating to have to withdraw from the work being conducted when it feels like there is more to be gained.
More positively, we recognise that we have also experienced opportunities for more thorough, in-depth ‘slow’ research, including the Sickle Cell project that this new article takes as its case study. We believe that this kind of ‘slow’ research, as previously explored in healthcare research by Vincanne Adams et. al (2013) and Heather Mendick (2014) amongst others, is an important antidote to the ever-building pressures that are heaped upon the researcher. To make things yet more complicated, these pressures come from a range of different external sources: for example, a rush to complete fieldwork within a limited timeframe to minimise costs for the funding body, or unexpected delays in participant recruitment that mean that tightly organised fieldwork cannot extend beyond the ethical clearance period granted by the host organisation.
This idea of ‘slow’ working isn’t new (see, for example, Honoré, 2005, or ‘A Call for Slow Scholarship’ by Hartman and Darab, 2012), but it is worth repeating: so much of academic research is subject to the restrictions of budget, outcome, time constraints and metrics that need ticking off that we forget how valuable time and space are for germinating our best ideas. The useful analytical frameworks, or new theories, or vital links we make between seemingly unrelated sets of results are often produced in the scarce time we get to think deeply about concepts or theories at length. It is this type of time which has become most compressed in the contemporary neoliberal university, where there are so many competing demands on the researcher’s time and attention, from emails to admin to marking to service.
In our discussions we came to a consensus that for us, 'slow' co-production is about having time to genuinely engage with others in dialogues that cover more ground than simply sharing ideas, although of course ideas come from dialogue so the two concepts aren't separate. As well as sharing ideas, we can think of slow co-production in terms of humanity and human rights: specifically, reducing the gap between the researcher and the researched, and trying to find common ground in a qualitative methodology that productively disrupts some of the traditional boundaries that we have seen replicated over and over across social sciences and public health research. Therefore, as well as the point that taking more time in the research field can develop more positive, meaningful relations between the different parties in the research, we also want to stress that this in-depth, detailed, sensitive approach to interviewing is a specific form of co-production, and one that we want to pursue further across our DEPTH projects.
So, whilst our article is primarily arguing for the importance of involving patients and participants in qualitative research from the start and throughout the lifespan of a research project, we hope it also offers a small insight into the opportunities enabled by ‘slow’, thorough working between researchers and participants. This ‘slow’ process – scarce as it sometimes feels the opportunity is – can offer a really valuable way into mutually beneficial collaboration.
References
Adams V, Burke NJ, Whitmarsh I. (2014) Slow Research: Thoughts for a Movement in Global Health. Medical Anthropology, 33(3): 179-97. https://doi.org/10.1080/01459740.2013.858335
Hartman Y, Darab, S. (2012) A Call for Slow Scholarship: A Case Study on the Intensification of Academic Life and Its Implications for Pedagogy. Review of Education, Pedagogy, and Cultural Studies, 34(1): 49-60. https://doi.org/10.1080/10714413.2012.643740
Honoré C. (2005) In Praise of Slowness: Challenging the Cult of Speed. New York: HarperCollins.
Mendick H. (2014) Social class, gender and the pace of academic life: What kind of solution is slow? Forum: Qualitative Social Research, 15(3):7. http://nbn-resolving.de/urn:nbn:de:0114-fqs140374.
Welcome to the introductory blog for the new website for our research group, DEPTH. We use the acronym DEPTH to bring together our research in Dialogue, Evidence, Participation and Translation for Health. We are a group of scholars in the Department of Public Health, Environments and Society at London School of Hygiene & Tropical Medicine who take an interdisciplinary approach to health. We conduct research into different types of dialogue and different people’s participation in health with the aim of increasing equity and improving health worldwide, and amplifying less-heard voices. Our new website aims to introduce a wider audience to our public health work. We see it as a space for communication and conversation – not just with academic colleagues, but also in policy debates, in education systems and with the wider public.
We think it is important to show our work to a wide range of audiences, not just specialists, and so we have listed all of our individual or combined efforts on this page, including summaries of each research paper listed in plain English, with concepts summarised and acronyms explained. You can read about the six Research themes that underpin DEPTH here. These research themes include our work on patient and public involvement, dialogues about sexual and reproductive health and young people’s experiences of Sickle Cell, and our work with Imperial College London on the ethics of electronic health records.
Finally, this regularly updated blog will provide a way for us to write about important studies in the field of community involvement, participation and public health. We will talk about our own research, but will also write about current affairs as well as research from elsewhere, when we would like to contribute to debate. We agree that one of the most important things we can do as academics is move beyond our own research specialisms to listen to – and amplify - the perspectives of those who may be less heard. We hope you will find these perspectives as valuable as we do.
We are excited to share with you this website as a portal to some of the pressing issues in sociologies of health. Community dialogue and participation is all about the exchange of ideas and synergies created by learning from each other. We can contribute the expert opinion, but we are just as interested in hearing from you. You can get involved via our new Twitter account, and you can contact us with questions, feedback or even your own blog pitch. Finally, look out for upcoming events on this blog page, where we will post details of future talks, meetings and events, as well as commentaries on new publications and policy.
Thanks again for reading and we look forward to sharing more about our work at DEPTH.
Cicely, Alicia, Catherine and Sam.

Non-technical summaries
Methods to measure effects of social accountability interventions in reproductive, maternal, newborn, child, and adolescent health programs: systematic review and critique
Marston, C, McGowan, C.R, Boydell, V, & Steyn, P.
Improving sexual and reproductive health and rights (SRHR) requires a wide range of approaches and measuring whether they work or not is obviously important to know how best to plan future efforts. Yet some approaches are very hard to measure adequately, for instance complex interventions aiming to improve social accountability, i.e. “…citizens’ efforts at ongoing meaningful collective engagement with public institutions for accountability in the provision of public goods”. In this paper, we searched for all the examples we could find of social accountability interventions where effects on SRHR were measured. In the paper we summarise all the different methods and data (qualitative and quantitative) used to measure effects of social accountability interventions on SRHR in the studies we found. The studies demonstrated the value of collecting qualitative data to help show whether and how interventions work, but the data and analysis were often limited in scope. There was little reported on theoretical frameworks guiding the interventions, almost no information about negative impacts of the interventions, and almost no information on costs or sustainability. We conclude that future studies should report on more areas relevant to policy (e.g. costs, sustainability, negative impacts), and should take into account broader socio-political dimensions to help illuminate processes of accountability and inform questions about likely usefulness of the interventions transferred to other contexts.
2020
Journal of Health, Population and Nutrition https://doi.org/10.1186/s41043-020-00220-z
Fertility and digital technology: narratives of using smartphone app ‘Natural Cycles’ while trying to conceive
Grenfell P., Tilouche N., Shawe J., & French, R.
Fertility awareness apps, which help approximate when conception is most likely, are increasingly popular. However, attention has typically focused on their use to prevent rather than help plan pregnancy. In the Freyja Study, we interviewed 24 cisgender women and 6 cismen in the UK about their experiences with one such app, Natural Cycles. Participants often valued the app as a ‘natural’ but ‘scientific’ alternative to biomedical interventions, that helped women get to know their bodies and feel control over the process. However, using the app required a structured routine, responsibility for which typically fell on women, and could intensify anxiety for those trying to conceive for longer. Some participants noted that the app’s advertising, cost and language created an image of ‘typical’ users as white, affluent, heterosexual, non-disabled, cisgender women. We conclude that, while fertility awareness apps may appeal as novel, empowering, natural and educational to people who use them, they can also exacerbate anxiety and reinforce power imbalances in relation to gender, race, class, disability, sexual and gender identity. We urge practitioners, app developers and researchers to attend to the mental as well as physical health implications of such technologies, and to the diverse needs, identities, realities and bodies of people who may want to use them. The Freyja Study was led by Dr Rebecca French from the Sexual Health & Reproductive Health Group.
2020
Sociology of Health & Illness
Unpacking power dynamics in research and evaluation on social accountability for sexual and reproductive health and rights
Schaaf, M, Cant, S, Cordero, J, Contractor, S, Wako, E, & Marston, C.
Social accountability for health has coalesced into a distinct field of research and practice. Whether explicitly stated or not, changed power relations are at the heart of what social accountability practitioners seek, particularly in the context of sexual and reproductive health. Yet evaluations of social accountability programs frequently fail to assess important power dynamics. In this paper, we argue that we must include an examination of power in research and evaluation of social accountability in sexual and reproductive health, and suggest ways to do this. The authors are part of a community of practice on measuring social accountability and health outcomes. We share key lessons from our efforts to conduct power sensitive research using different approaches and methods. We note that failing to engage questions of power in sexual and reproductive health interventions – which can be highly politicised – risks undermining attempts to improve health and rights by locating problems solely in individual behaviour or characteristics that need to be fixed, glossing over the impact of political structures and entrenched social hierarchies. While these structures and hierarchies are resistant to change, they are at the heart of what must change to meaningfully improve sexual and reproductive health.
2021
International Journal for Equity in Health, https://doi.org/10.1186/s12939-021-01398-2
Understanding the health-care experiences of people with sickle cell disorder transitioning from paediatric to adult services: This Sickle Cell Life, a longitudinal qualitative study
Renedo, A; Miles, S; Chakravorty, S; Leigh, A; Warner, J. O.; Marston C.
In our NIHR report for ‘This Sickle Cell Life’, we argue that what happens during transitions from childhood to adulthood affects young people’s future lives. Sickle cell disorder is one long-term condition for which transitions are particularly challenging and people’s health can suffer. We interviewed young people with sickle cell disorder and sickle cell specialist healthcare providers in England and found that during transition young people aren’t always listened to by healthcare providers or recognised as experts in their own condition. As a result, young people avoid going to places where they have not experienced good care, such as A&E departments and on general wards, even though they know that avoiding hospital is risky. We need to support others in young people’s social and health-care environments to learn about sickle cell disorder and to treat young people as experts in their own condition.
2020
NIHR Health Services and Delivery Research Volume 8, Issue 44
Community participation is crucial in a pandemic
Marston, C; Renedo, A; Miles, S.
We argue that community participation is essential in the collective response to the COVID-19 pandemic. We set out how community engagement has the potential to address a range of government and public health needs, including encouraging public compliance with social restrictions and prevention measures, community support through volunteering, and mutual aid – from the immediate neighbourhood right up to the national or international level. We urge health professionals to work together with communities to plan, deliver, and evaluate the best possible health promotion and health-care services, and note that this is particularly important in a crisis – especially one that is likely to be prolonged and involve major social and political responses. Governments and health bodies must take steps to ensure citizen participation; we set out steps needed to achieve this: invest in coproduction, work with community groups, commit to diversity, and be responsive and transparent. Finally, we conclude that good public participation will reveal policy gaps and the potential negative consequences of emergency responses, and that this in itself helps us to find ways to address these issues together.
2020
The Lancet, DOI: https://doi.org/10.1016/S0140-6736(20)31054-0
Inviting the stranger in: Intimacy, digital technology and new geographies of encounter
Koch, R; Miles, S.
In this paper we argue that digital technologies are having a big impact on how people meet each other and that we do not know enough about what these encounters are like or how they should be researched. We study GPS-enabled apps for sex and dating such as Tinder and Grindr, as well as sharing economy apps such as Uber, AirBnB and SpareRoom, to show how technology is making encounters between strangers more private than public as time goes on. We term this stranger intimacy, showing how it can develop knowing, providing, befriending or even loving between people. We also look at who gets included and excluded in these kinds of new intimacies, and who is privileged or disadvantaged. We conclude by setting an agenda for future study of digital technology and intimacy that researchers may want to consider.
2020
Progress in Human Geography DOI:10.1177/0309132520961881
Communicating and understanding pain: Limitations of pain scales for patients with sickle cell disorder and other painful conditions
Collins, P; Renedo, A; Marston, C.
For hospital patients, talking about pain can be difficult. We look at the use of pain scales (where a patient rates their pain from 1-10 to communicate how severe pain is) using a case study of people with sickle cell disorder (SCD). Our findings show there are important social and contextual influences on how patients express pain and how providers interpret it. When talking about pain, participants often introduced significant others (e.g. parents or family) into their narratives, prioritising others’ feelings and experiences of their painful episodes. When it comes to sickle cell disorder, mutual distrust shapes pain communication, and further complicates assessments by healthcare staff. On top of this, SCD pain is particularly severe: this makes ratings hard to interpret compared with ratings from non-SCD patients. This in turn may lead to problems in managing pain relief and prescribing medication.
2020
Journal of Health Psychology, DOI: 10.1177/1359105320944987
Not being heard: barriers to high quality unplanned hospital care during young people’s transition to adult services – evidence from ‘this sickle cell life’ research
Renedo, A; Miles, S; Chakravorty, S; Leigh, S; Telfer, P; Warner, J & Marston, C.
In this article we explore how young people with sickle cell disease experience healthcare during the period of transition – the time from when a young person prepares to move into adult healthcare services until the person is fully adjusted to adult services. We conducted 80 interviews across England with 48 young people with sickle cell disease aged between 13 and 21. We focused on their experiences of healthcare outside specialist sickle cell clinics, such as A&E. We found that young people reported problems with both the care they received in A&E during painful episodes, and in hospital wards as inpatients. They were not listened to by non-specialist hospital staff, nor recognised as experts in their own condition. They experienced delays in being given pain relief. Because of their experiences, young people tried to avoid going to hospital, attempting to manage their pain at home and going to hospital for a painful episode only as a last resort. Our study highlights the need for improvements to make services youth-friendly and to act on young people’s voices to ensure they are involved in shaping their own healthcare. We also argue that training staff in sickle cell disease-specific care is key to young people's well-being.
2019
BMC Health Services Research, https://doi.org/10.1186/s12913-019-4726-5
Transitions to adulthood: self‐governance and disciplining in the making of patient citizens
Renedo, A; Miles, S; Marston, C.
When young people move from child to adult health services they redefine their identities, but we don’t yet know enough about how these transitions shape identities. Our interviews with young people with sickle cell disease explored how they define new identities as they transition to adulthood. We show that health transitions are tricky for young people, who have to balance competing demands for self‐discipline: to stay healthy while working hard to become successful adults in other areas of their life. The development of adult identities for young people with SCD can be exhausting, involving relentless self-disciplining and self-monitoring in different aspects of life. They see themselves as in constant need of improvement. We conclude that it is crucial to create enabling spaces for young people to protect their health while still developing identities that help them achieve life goals.
2019
Sociology of Health & Illness, https://doi.org/10.1111/1467-9566.13019
Neglect of STIs and infertility undermines family planning programmes
Marston, C & Francis, S.
Neglect of STIs and infertility undermines family planning programmes worldwide. One reason that people still do not use effective contraception methods is because many women and their families in low- and middle-income countries fear the most effective contraceptives can cause infertility. A conventional response to this is that people simply need more information to put them on the right track. However, the article argues that there is infertility risk in some settings from undiagnosed, asymptomatic STIs, particularly chlamydia. Uncontrolled chlamydia epidemics have recently been identified that may well be causing infertility, including among women who have stopped using contraceptives. This may cause people to worry the contraceptives caused the infertility as they are unaware of the STI infection. Marston and Francis conclude that recent studies in South Africa indicate the scale of the threat STIs pose to women’s fertility, and suggest that this problem, and any resulting infertility, is likely not confined to one country. Treating infertility should be part of a people-centred family planning programme. Counterintuitively, taking infertility seriously and addressing it might even increase uptake of contraception by improving trust that contraception is not the cause of the infertility. Failing to consider real concerns about infertility, on the other hand, is likely to undermine family planning programmes.
2019
BMJ Sexual & Reproductive Health, DOI: https://doi.org/10.1136/bmjsrh-2018-200270
Exploring stigma and social norms in women’s abortion experiences and their expectations of care
Makleff S, Wilkins R, Wachsmann H, Gupta D, Wachira M, Bunde W, Radhakrishnan U, Cislaghi B, Baum SE.
In this study we show how women having abortions in Kenya and India have quite similar fears and expectations for their abortion service, despite major differences in the legal and social contexts in the two countries. In Kenya, abortion is permitted under limited conditions, and there are many barriers to access, including confusion about whether abortion is actually legal. In India, abortion is legal and accessible up to 20 weeks of gestation with few restrictions, though many women still access care outside the formal health system. In both these settings, we found that women arrived for their abortion with little accurate knowledge, negative attitudes towards abortion, fears about the safety and side effects, concerns about being judged, and low expectations for how they would be treated during their abortion. Younger women in both countries expressed particularly strong concerns about abortion safety, potentially because they were scared to look for information or support. Our findings suggest that young women (particularly in Kenya) and unmarried women (particularly in India) are more likely to experience abortion stigma. We propose that clinics in both countries could develop strategies to promote access to youth-friendly services and consider how to reduce experiences of abortion stigma and improve women’s expectations of abortion services – this would ultimately help improve client-centred care.
2019
Sexual and Reproductive Health Matters, 27:3, 1661753, DOI: 10.1080/26410397.2019.1661753
Obstacles to use of patient expertise to improve care: a co-produced longitudinal study of the experiences of young people with sickle cell disease in non-specialist hospital settings
Miles, S; Renedo, A; Augustine, C; Ojeer, P; Willis, N & Marston, C.
In this paper, co-produced between academic researchers and people with lived experiences of sickle cell, we examine how young people with sickle cell disease try to use their expertise in their own condition during emergency hospital admissions and through encounters with healthcare workers who are not sickle cell specialists. Our qualitative research in England examined young people’s experiences of hospital encounters through repeat and one-off interviews. We show that young people’s expertise is sometimes undermined, including not being taken seriously when they report pain. They face barriers to care in non-specialist wards, particularly when they are alone with nobody to advocate for them. Although healthcare services encourage young people to take control of their health as ‘patient experts’, in practice young people’s expertise is routinely ignored. To improve health service quality and young people’s needs, their own expertise must be better supported by healthcare providers.
2019
Critical Public Health, DOI: 10.1080/09581596.2019.1650893
Going the Distance: Locative Dating Technology and Queer Male Practice-Based Identities
Miles, S.
Sam’s chapter in The Geographies of Digital Sexuality explores the practices of men seeking men on online dating apps. He argues that these practices can be categorised into different identities or ‘type’ of user. The chapter uses narratives from real-life qualitative interview data to develop three profiles: the Embracer, the Timewaster, and the Minimalist. These ‘types’ are not fixed, but instead flexible categorisations that users might adopt, consciously or not, at different times in their app use over time. The strong feelings that the three defined profiles provoke for other apps users shows that the social codes of GPS-enabled apps have yet to catch up to their digital sophistication. This can help us to think about larger questions beyond dating apps, like who we ‘are’ when we’re online, and why that still feels disembodied from what should by now be a more taken-for-granted, hybridised digital-physical life.
2019
The Geographies of Digital Sexuality, pp 115-135. https://doi.org/10.1007/978-981-13-6876-9_7
Citizen Participation in Neoliberal Times
Komporozos-Athanasiou, A, Renedo, A, McKevitt, C.
In this introduction to the Special Issue on Citizen Participation in Neoliberal Times, we invite readers to critically think about the concept of citizen participation and approach it from different disciplinary lenses. We briefly introduce the different publications of the special issue and reflect on the conceptual contributions these make. Ideas include a new way to think about how we engage with children’s voices in participatory work, through to understanding participation as a process through which citizens can be empowered to produce new forms of knowledge to address issues that affect their life, that if not done well risk being ‘shaped’ into particular types of people, such as ‘responsible’ patients who avoid risks and fulfil official public health targets.
2019
Sociological Research Online, 0(0):1360780419835562
“I've never told anyone this before”: Co‐constructing intimacy in sex and sexualities research
Miles, S.
How do researchers go about interviewing people about sensitive topics, including sex and sexuality? In this article, Sam Miles explores how researcher and participant can work together to create or ‘co-produce’ a safe, non-judgemental space for honest talking. He reflects on how involved a researcher should be in this space and the ethical boundaries of becoming too involved in participants’ lives. He also questions the extent to which we should share our own experiences as researchers. He argues that an appropriate space for participant disclosure can be public and one-off, rather than private or a relationship which depends on repeated meetings. The paper concludes that assumption that private matters cannot be discussed in public requires a rethink.
2019
AREA, DOI: 10.1111/area.12550
Preventing Intimate Partner Violence Among Young People - a Qualitative Study Examining the Role of Comprehensive Sexuality Education
Makleff, S; Garduño, J, Zavala RI; Marston, C.
It seems likely that comprehensive sexuality education may help prevent intimate partner violence, but few studies have examined this. In this article, we explore the ways that a “gender-transformative” comprehensive sexuality education course in Mexico City may help prevent intimate partner violence. We conducted in-depth interviews and focus groups with students ages 14 to 17 as well as their teachers and health educators. The data suggest that the comprehensive sexuality education course helped young people develop strategies to prevent and respond to partner violence. We found four elements of the course that seem central to violence prevention. First, encouraging young people to reflect about romantic relationships, which helped them question whether jealousy and possessive behaviors are signs of love; second, helping them develop skills to communicate about sexuality, inequitable relationships and reproductive health; third, encouraging care-seeking behavior; and fourth, addressing norms around gender and sexuality, for example demystifying and decreasing discrimination towards sexually diverse populations. The results suggest that this promising and relatively short-term intervention should be considered as a school-based strategy to prevent and respond to partner violence.
2019
Sexuality Research and Social Policy, https://doi.org/10.1007/s13178-019-00389-x
Surviving Ebola: A historical cohort study of Ebola mortality and survival in Sierra Leone 2014-2015
Wing, K; Oza, S; Houlihan, C; McGowan, C.
Various predictors for Ebola mortality have been identified but less is known about post-viral symptoms. Identification of acute-illness predictors for post-viral symptoms could allow the selection of patients for more active follow up in the future, and those in whom early interventions may be beneficial in the long term. Studying predictors of both mortality and post-viral symptoms within a single cohort of patients could also further our understanding of the pathophysiology of survivor sequelae. We performed a historical cohort study using data collected as part of routine clinical care from an Ebola Treatment Centre (ETC) to identify predictors of mortality and of post-viral symptoms. Our findings may add epidemiological support to the hypothesis that post-viral symptoms have an immune-mediated aspect and may not only be a consequence of high viral load and disease severity.
2018
PLOS ONE, https://doi.org/10.1371/journal.pone.0209655
Still getting it on online: Thirty years of queer male spaces brokered through digital technologies
Miles, S.
In this article, Sam Miles argues that the advent of the internet has been the biggest single impact on queer space over the last thirty years. The article reviews research that tracks the relationship between queerness and digital technology, from online chatrooms to desktop-based dating portals, and most recently GPS-enabled smartphone dating apps. Miles argues that queer spaces have become increasingly dominated by internet technology, and this has positive, as well as more ambiguous, effects on how men seeking men choose to meet and pursue social and sexual relationships. The huge popularity of apps including Grindr and Tinder mix online and offline space into a hybrid experience. This hybridisation has implications for wider technology use and social interaction for a whole range of people who use technology in their daily lives.
2018
Geography Compass, ISSN 1749-8198 DOI: https://doi.org/10.1111/gec3.12407
Slow co-production' for deeper patient involvement in health care
Miles, S; Renedo, A; Marston, C.
In this paper we argue that in-depth qualitative research can be seen as a way to engage in ‘slow co-production’. Involving patients from the start and throughout a piece of research, and ensuring their voices are central can help deepen patient involvement in healthcare. We use our qualitative research project This Sickle Cell Life as a study to demonstrate how working in depth with patients can generate detailed data for researchers and patient-centred knowledge that can help improve health services.
2018
The Journal of Health Design, 3 (1). pp. 57-62. ISSN 2206-785X DOI: https://doi.org/10.21853/JHD.2018.39
Pornography and young people’s health: evidence from the UK sixteen18 project
Marston, C.
In this short paper, Cicely Marston presents evidence from the recent LSHTM ‘sixteen18’ research project into young people’s sex lives. The project explored a range of sexual behaviours and attitudes; this paper focuses specifically on pornography. The paper argues that there is little evidence to support claims that porn is a public health danger, contrary to political and media coverage of young people in particular. The sixteen18 project did indicate some harms from using pornography as ‘sex education’, which suggests that sexuality education should emphasize the importance of mutuality and consent, but argues that sexual coercion and consent are better understood within the larger cultural context. Future research using an interdisciplinary and especially ethnographic approach can build up a holistic picture of porn use and health effects.
2018
Porn Studies, pp. 1-4. ISSN 2326-8743 DOI: https://doi.org/10.1080/23268743.2018.1434153
Setting the research agenda for induced abortion in Africa and Asia
Scott, RH; Filippi, V; Moore, AM; Acharya, R; Bankole, A; Calvert, C; Church, K; Cresswell, JA; Footman, K; Gleason, J; Machiyama, K, Marston, C; Mbizvo, M, Musheke, M, Owolabi, O, Palmer, J, Smith, C, Storeng, K, and Yeung, F.
Safe abortions are vital for ensuring the health and wellbeing of populations across the world, and research on abortion is essential to meet the UN Sustainable Development Goals. In this article, we report on the recommendations from a workshop for researchers working on contraception and abortion in Africa and Asia to discuss future abortion research. We argue that there is great untapped potential in designing intervention strategies including clinical innovations, quality improvement work, and involving local communities. Research with specific groups, including adolescents and young people, men, populations affected by conflict, and marginalized groups could increase understanding of provision, access to and experiences of induced abortion, in turn improving experiences of induced abortion in Africa and Asia.
2018
International journal of gynaecology and obstetrics, ISSN 0020-7292 DOI: https://doi.org/10.1002/ijgo.12525 Item availability may be restricted.
Improving the Measurement of Fertility Regulation Practices: Findings from Qualitative Research in Ghana
Marston, C; Renedo, A; Nyaaba, GN; Machiyama, K; Tapsoba, P; Cleland, J.
This article digs deeper into the question of why demographic data on highly educated urban woman in Ghana suggest, counter-intuitively, that they have low rates of both contraceptive use and fertility. Individual interviews and focus group discussions with women on contraception, reproduction and fertility regulation strategies showed that women often combine contraception methods, including calendar methods, withdrawal, condoms and emergency contraception. This in-depth data illustrates how they use contraception in more detail than a large-scale survey can manage. The article concludes that new ways of capturing women's complex fertility regulation practices should be considered, including additional survey items, new questions and specialist studies.
2018
International Perspectives on Sexual and Reproductive Health, 43 (3). pp. 111-119. ISSN 1944-0391 DOI: https://doi.org/10.1363/43e4517
Fertility regulation as identity maintenance: Understanding the social aspects of birth control
Marston, C; Renedo, A; Nyaaba, GN.
In this article about the social aspects of birth control in West Africa, we take a narrative-based approach to exploring how women regulate their fertility, and we show how they can maintain or express social identity. We identify three themes in educated Ghanaian women's accounts of how they navigate social demands on their identity when trying to regulate their fertility: secrecy and silence (hiding contraception and avoiding talking about it); tolerating uncertainty (for example using unreliable but more socially acceptable contraception); and wanting to be fertile. The article concludes that family planning programmes that fail to tackle these obstacles to regulating fertility will risk reproducing social spaces where women struggle to claim their reproductive rights.
2017
Journal of health psychology, p. 1359105317726367. ISSN 1359-1053 DOI: https://doi.org/10.1177/1359105317726367
The co-production of what? Knowledge, values, and social relations in health care
Filipe, A; Renedo, A; Marston, C.
Co-production is becoming a buzzword in healthcare settings. This article, published in PLOS Biology (2017), argues that the concept does not always explain what the implications of co-production might be for participants (or healthcare users more widely). We argue that co-production can be thought of as a process that encourages new ways of thinking about collaboration and participation in healthcare.
2017
PLOS Biology, 15 (5). e2001403. DOI: https://doi.org/10.1371/journal.pbio.2001403
Experience as Evidence: The Dialogic Construction of Health Professional Knowledge through Patient Involvement
Renedo, A; Athanasiou, A; Marston, C.
How can we advance knowledge through patient and public involvement? The relationship between healthcare professionals and patients is crucial. This article, published in Sociology (2017), draws on ethnographic work on patient involvement. We show how new knowledge is produced when professionals engage with patients, particularly in how healthcare professionals articulate the relationship between ‘subjective’ patient experience and ‘objective’ evidence.
2017
Sociology, ISSN 0038-0385 DOI: https://doi.org/10.1177/0038038516682457
Factors affecting effective community participation in maternal and newborn health programme planning, implementation and quality of care interventions
Howard-Grabman, L; Miltenburg, AS; Marston, C; Portela, A.
How can we enhance how communities get involved in service improvements? In this article, published in BMC Pregnancy & Childbirth (2017), we examine the factors affecting implementation of community participation strategies in maternal and newborn health programmes. We find that community participation is stronger where communities see women’s health as a collective responsibility, and where participation is linked into a functioning health system (such as via user groups). We suggest that viewing participation as an ongoing process is crucial to effective participation, as is focusing on creating an environment that enables communities to participate in improving health.
2017
BMC Pregnancy and Childbirth, DOI: 10.1186/s12884-017-1443-0
Improving implementation of health promotion interventions for maternal and newborn health
Smith, HJ; Portela, AG; Marston, C.
In this overview article for the BMC Pregnancy and Childbirth series on maternal and newborn health promotion, we present evidence that health promotion interventions may not achieve their objectives because they fail to engage with beneficiaries and the community. We argue that with better formative research, programmes can implement interventions to help individuals and communities access skilled care in pregnancy and childbirth. A participatory approach is key to this success.
2017
BMC Pregnancy Childbirth, 17 (1). p. 280. ISSN 1471-2393 DOI: https://doi.org/10.1186/s12884-017-1450-1
Oral Sex, Young People, and Gendered Narratives of Reciprocity
Lewis, R; Marston, C.
This paper looks beyond gender differences amongst young people in giving and receiving oral sex to explore their own perspectives on gender dynamics in oral heterosex. Here, we explore the stories told by 16-18 year old men and women in England in their accounts of oral sex via in-depth interviews. On one hand, oral sex on men and women was narrated as equivalent, while on the other, oral sex on women was seen as “a bigger deal” than oral sex on men. Young men and women used a ‘give and take’ discourse to make oral sex ‘fair’. We argue that ostensibly positive discourses about equality in sexual practices also obscure women’s constrained agency and work in giving oral sex.
2016
Journal of sex research, 53 (7). pp. 776-87. ISSN 0022-4499 DOI: https://doi.org/10.1080/00224499.2015.1117564
Does the evidence support global promotion of the calendar-based Standard Days Method® of contraception?
Marston, CA; Church, K.
This article examines claims about the effectiveness of the Standard Days Method® (SDM), marketed as a modern contraceptive method used in at least 100 countries worldwide. Its claim that it is 95% effective when used correctly is repeated in recent documents from the World Health Organization. We find that existing evidence does not support claims that the effectiveness of SDM as promoted is comparable to the best short-acting modern contraceptive methods. SDM is promoted in ways that may mislead users, by quoting overestimates of effectiveness and providing efficacy comparisons only with selected methods of contraception. We conclude that delivery of any form of SDM should include accurate effectiveness information as well as presentation of the full range of other contraceptive methods, including the most effective options.
2016
Contraception, 93 (6). pp. 492-7. ISSN 0010-7824 DOI: https://doi.org/10.1016/j.contraception.2016.01.006
Community participation for transformative action on women's, children's and adolescents' health
Marston, C; Hinton, R; Kean, S; Baral, S; Ahuja, A; Costello, A; Portela, A.
Community participation can transform health. The Global Strategy for Women’s, Children’s and Adolescents’ Health recognizes that people have a central role in improving their own health. In this article we propose that community participation, including communities working with health services (‘co-production’), will be central for achieving the objectives of the Global Strategy. The paper addresses the role of community participation in promoting health and wellbeing for women, children and young people. We argue that contextualised community participation that is inclusive of under-served groups optimises interventions to improve health. This action relies on participatory approaches that build new relationships across the health system.
2016
Bulletin of the World Health Organization, 94 (5). pp. 376-82. ISSN 0042-9686 DOI: https://doi.org/10.2471/BLT.15.168492
The use of information for diabetes research and care: patient views in West London
Zalin, A; Papoutsi, C; Shotliff, K; Majeed, A; Marston, C; Reed, J.
This study explores the public views on use of electronic health records, finding that people with diabetes would like personal access to such records, and for their medical history to be captured in full. The majority also supported use of their health records for research. The findings support the idea that patients believe in sharing their data for the ‘greater good’.
2016
Practical Diabetes, 33 (3). 81-86a. ISSN 2047-2900 DOI: https://doi.org/10.1002/pdi.2008
Developing patient-centred care: an ethnographic study of patient perceptions and influence on quality improvement
Renedo, A; Marston, C.
Patient-centred care relies on understanding quality improvement from the perspective of the patient, yet patients are often excluded from this process. In this BMC Health Services Research (2015) article, we explore how patients view quality improvement and how they go about improving health services. The article demonstrates how expectations around who the patient is and how they should behave as a recipient of care can influence how patients negotiate their rights to quality care. For genuine involvement in healthcare, it is important to work with patients to reflect on how neoliberal ideas around personal responsibility might influence how and whether patients demand quality care.
2015
BMC Health Services Research, 15. p. 122. ISSN 1472-6963 DOI: https://doi.org/10.1186/s12913-015-0770-y
Patient and Public Involvement in Healthcare Quality Improvement: How organizations can help patients and professionals to collaborate
Renedo, A; Marston, CA; Spyridonidis, D; Barlow, J.
Given that patient participation can improve healthcare, how can organisations help patients and professionals to collaborate? In this article in Public Management Review (2015), we suggest that the ways citizens can participate in healthcare improvement is often unclear, and we highlight how patients can be supported to make an impact. Our findings demonstrate that patients can influence healthcare beyond just providing their views as receivers of care. We draw on ethnographic work within a UK healthcare initiative and outline how patients can use elements of organisational culture to help them collaborate with health professionals for better outcomes.
2015
Public Management Review, 17 (1). pp. 17-34. ISSN 1471-9037 DOI: https://doi.org/10.1080/14719037.2014.881535 Full text not available from this repository.
Patient and public views about the security and privacy of Electronic Health Records (EHRs) in the UK: results from a mixed methods study
Papoutsi, C; Reed, JE; Marston, C; Lewis, R; Majeed, A; Bell, D.
This article examines claims about the effectiveness of the Standard Days Method® (SDM), marketed as a modern contraceptive method used in at least 100 countries worldwide. Its claim that it is 95% effective when used correctly is repeated in recent documents from the World Health Organization. We find that existing evidence does not support claims that the effectiveness of SDM as promoted is comparable to the best short-acting modern contraceptive methods. SDM is promoted in ways that may mislead users, by quoting overestimates of effectiveness and providing efficacy comparisons only with selected methods of contraception. We conclude that delivery of any form of SDM should include accurate effectiveness information as well as presentation of the full range of other contraceptive methods, including the most effective options.
2015
Bmc Medical Informatics and Decision Making, 15. ISSN 1472-6947 DOI: https://doi.org/10.1186/s12911-015-0202-2
Patient and public attitudes towards informed consent models and levels of awareness of Electronic Health Records in the UK
Riordan, F; Papoutsi, C; Reed, JE; Marston, C; Bell, D; Majeed, A.
Electronic Health Records (EHRs) are key to NHS services because they facilitate health information for both patient care and secondary research. Using questionnaire surveys in London clinics, this project explored public awareness about EHRs and examined attitudes towards different consent models with respect to sharing patient records for healthcare and research. We found that most respondents expected to be asked for consent for their records to be used, and that over half of participants were aware of EHRs before the survey. However this means that many are unaware of EHRs, so education campaigns are needed to increase public awareness and ensure meaningful informed consent.
2015
International journal of medical informatics, 84 (4). pp. 237-47. ISSN 1386-5056 DOI: https://doi.org/10.1016/j.ijmedinf.2015.01.008
Conceptualising the 'community' as a recipient of money - A critical literature review, and implications for health and inequalities
Reynolds, J; Egan, M; Renedo, A; Petticrew, M.
Money may bring about positive changes to health, and giving money to ‘the community’ is becoming more common. This article reviews how governments in different countries give money to the community, exploring how community is conceptualised in this set-up. The article highlights the need for a better understanding of how money affects health and how community is not just a recipient of money, but also something that is constructed through the act of giving money.
2015
Social science & medicine, 143. pp. 88-97. ISSN 0277-9536 DOI: https://doi.org/10.1016/j.socscimed.2015.08.049
WHO recommendations on health promotion interventions for maternal and newborn health
Portela A, Smith H, Marston C.
The LSHTM team provided technical expertise for this World Health Organization recommendation in 2015 on health promotion interventions for maternal and newborn health. The recommendations help countries to establish how best to increase individual, family and community capacity to contribute to maternal and newborn health improvements and skilled care during pregnancy and birth. Recommendations include enhancing community participation in service planning and quality improvement.
2015
World Health Organisation: Maternal, newborn, child and adolescent health. http://www.who.int/maternal_child_adolescent/documents/health-promotion…;
Anal heterosex among young people and implications for health promotion: a qualitative study in the UK
Marston, C; Lewis, R.
In this paper we set out to explore expectations, experiences and circumstances of anal sex among young people, through qualitative interviews with individuals and groups in three different settings in England. We found that anal heterosex often appeared to be painful, risky and coercive, particularly for women. Interviewees frequently related anal sex to pornography, but in fact pornography seemed to only make up part of the practice. Other elements included normalisation of pressure to have anal sex, and ‘accidental’ penetration. Our study suggests an urgent need to reduce coercive, painful and unsafe anal heterosex; we want to encourage discussion about shared desire and consent, reduce risky and painful techniques and challenge views that normalise coercion.
2014
BMJ Open, 4 (8). e004996. ISSN 2044-6055 DOI: https://doi.org/10.1136/bmjopen-2014-004996
Spaces for Citizen Involvement in Healthcare: An Ethnographic Study
Renedo, A; Marston, C.
This theoretical contribution to Sociology (2014) considers participation and involvement in healthcare in terms of the spaces in which these activities take place. We develop the idea of “participatory spaces” with material, temporal and social dimensions, and argue that paying attention to these is important to understand the dynamics and impact of patient involvement. We show how participants play a crucial role, drawing on external resources to try and make participatory spaces more collaborative and productive, which helps build a more positive landscape for healthcare. We also highlight how spaces created for public involvement can hinder patients trying to shape healthcare. Only certain social groups can participate, and their influence is limited when they find participatory spaces difficult to navigate.
2014
Sociology, DOI: https://doi.org/10.1177/0038038514544208
WHO recommendation on community mobilization through facilitated participatory learning and action cycles with women’s groups for maternal and newborn health
Marston C, Portela A.
The LSHTM team provided technical expertise for this World Health Organization recommendation on community mobilisation through participatory learning and action cycles with women’s groups for maternal and newborn health. In the report, we set out the importance of interventions in improving maternal and newborn health, family care, community support, and access to skilled care.
2014
World Health Organisation: Maternal, newborn, child and adolescent health. http://www.who.int/maternal_child_adolescent/documents/community-mobili…;
Effects of community participation on improving uptake of skilled care for maternal and newborn health: a systematic review
Marston, C; Renedo, A; McGowan, CR; Portela, A.
Our systematic review of the effects of community participation on improving the uptake of skilled care for maternal and newborn health examines the extent to which participation improves maternal and newborn health outcomes. We draw on this literature and our own work to set out new theoretical and reporting frameworks to help guide future research.
2013
PLoS One, 8 (2). e55012. ISSN 1932-6203 DOI: https://doi.org/10.1371/journal.pone.0055012
Patient and public views on UK electronic health record systems and their uses: cross-sectional survey
Luchenski, S; Reed, J; Marston, C; Papoutsi, C; Majeed, A; Bell, D.
Implementation of electronic health records (EHRs) remains a challenge; finding out more about patient and public attitudes to EHRs is needed to inform policy. This article explores patient and public attitudes towards EHRs using a survey, and finds that despite previous difficulties with NHS technology projects, patients and members of the public generally support the development of integrated EHRs for health care provision, planning and policy, and health research.
2013
Journal of medical Internet research, 15 (8). e160. ISSN 1439-4456 DOI: https://doi.org/10.2196/jmir.2701
Increasing the use of skilled health personnel where traditional birth attendants were providers of childbirth care: a systematic review
Vieira, C; Portela, A; Miller, T; Coast, E; Leone, T; Marston, C.
Recognising that improved access to skilled health personnel is key to improving maternal health, this study investigates how this has been achieved where traditional birth attendants helped with childbirth. We find that interventions that increase the use of skilled care lead to positive outcomes on maternal health, but other factors in childbirth scenarios need consideration too, including distance, travel, and family preferences in what healthcare interventions are performed. We also find that that there are few high-quality studies that measure effectiveness of these interventions.
2012
PLoS One, 7 (10). e47946. ISSN 1932-6203 DOI: https://doi.org/10.1371/journal.pone.0047946
Survey of patient and public perceptions of electronic health records for healthcare, policy and research: Study protocol
Luchenski, S; Balasanthiran, A; Marston, C; Sasaki, K; Majeed, A; Bell, D; Reed, JE.
The benefits of a national electronic health records (EHR) system must be balanced against public concerns about security and privacy. Our EHR study explores the correlation between personal healthcare experience (including number of healthcare contacts and number and type of longer term conditions) and views relating to development of EHRs. The study design and implementation were successful, with unusually high response rates.
2012
BMC Med Inform Decision Making, 12. p. 40. ISSN 1472-6947 DOI: https://doi.org/10.1186/1472-6947-12-40
Healthcare Professionals' Representations of 'Patient and Public Involvement' and Creation of 'Public Participant' Identities: Implications for the Development of Inclusive and Bottom-Up Community Participation Initiatives
Renedo, A; Marston, C.
Community participation, particularly “patient and public involvement”, is seen as important to improving healthcare, but what does it mean? In this foundational article for Community and Applied Social Psychology (2011), we draw on UK ethnographic research to explore how patient understandings of their own involvement in healthcare are influenced by relationships with healthcare providers and their expectations about the role of a patient. We argue that patients may struggle to achieve change without support from professionals, and that these relationships must be examined and developed if successful community participation is to happen.
2011
Journal of community & applied social psychology, 21 (3). pp. 268-280. ISSN 1052-9284 DOI: https://doi.org/10.1002/casp.1092
Alicia Renedo
Associate Professor, Lead researcher
Casey Lynn
Crow
PHP - DL Tutor

Catherine
McGowan
Associate Professor
Charlotte Kuhlbrandt
Researcher, Routes project
Cicely
Marston
Honorary Professor of Public Health
Joelle
Mak
Assistant Professor
Laura Dix
Project Manager
Marthe LePrevost
Research Degree Student
Mary Mbuo
Research Degree Student
Pippa
Grenfell
Associate Professor
Prima Alam
Research Degree Student
Rachel Stuart
Researcher, Routes project

Rebecca
Blaylock
Research Fellow
Sam Miles
Assistant Professor
Shelly Makleff
Research Degree Student
